![Brain Under Pressure – A Guide to Understanding Intracranial Hypertension [Updated]](https://staging.chiaribridges.org/wp-content/uploads/2019/12/Woman_Up-with-headache_AS177290930.jpg)
INTRACRANIAL HYPERTENSION (IH) MEANS HIGH PRESSURE INSIDE THE SKULL.
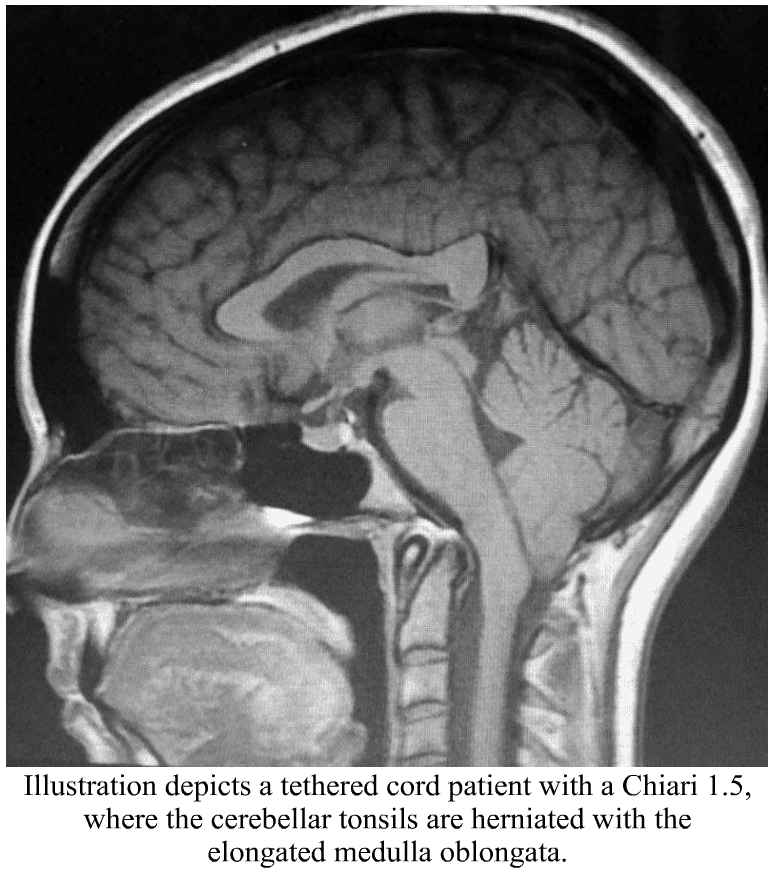
Intracranial Pressure (ICP) is measured in millimeters of mercury (mmHg). Most scholars agree that on average, “normal pressure” should be between 5-15 mmHg, mild to moderate intracranial hypertension between 20-30 mmHg (which “requires treatment in most circumstances”), and an ICP of > 40 mmHg indicates “severe and possibly life-threatening intracranial hypertension.” [1] When high intracranial pressure is left untreated, it creates a “pushing effect” towards the only natural escape at the base of the skull (the foramen magnum), and the cerebellar tonsils in the pathway are pushed through the foramen magnum. [2]
Understanding the Monro-Kellie Doctrine (pressure-volume relationship)
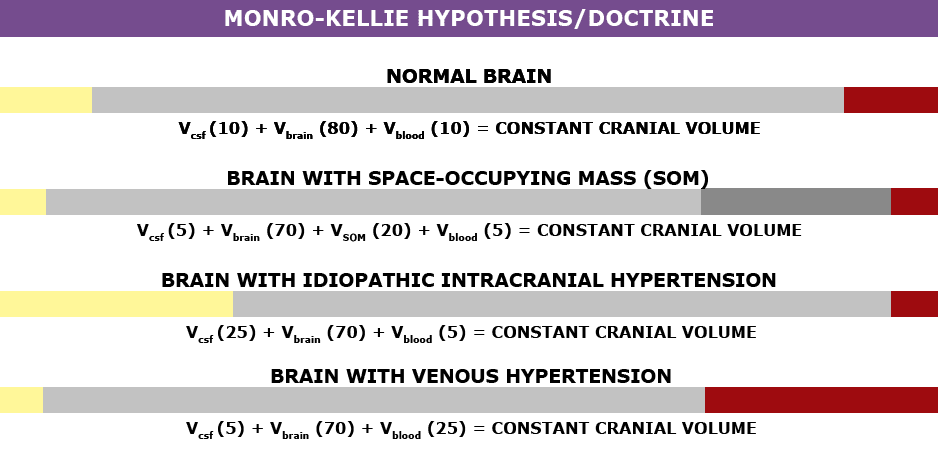 The association between IH/IIH and Chiari Malformation appears to be a malicious intricate pathological circle. The cranium (skull) consists of brain matter, cerebrospinal fluid, and both venous and arterial blood. A hypothesis, referred to as the Monro-Kellie Hypothesis (now better known as the Monro-Kellie Doctrine), states, “The sum of volumes of the brain, CSF, and intracranial blood is constant. An increase in one should cause a decrease in one or both of the remaining two.” Therefore, if an abundance of cerebrospinal fluid (IIH or hydrocephalus), both cranial blood volume and brain matter should be forced to deplete. This depletion is usually directed in the path of least resistance – through the foramen magnum and into the spinal canal. When the brain matter closest to the bottom of the skull (cerebellar tonsils) is pushed through the foramen magnum and into the spinal canal (an Acquired Chiari Malformation), the tonsils act like a cork and blocks the flow of cerebrospinal fluid (regardless of the size of the tonsillar descent), which in turn, continues to raise intracranial pressure.[3]
The association between IH/IIH and Chiari Malformation appears to be a malicious intricate pathological circle. The cranium (skull) consists of brain matter, cerebrospinal fluid, and both venous and arterial blood. A hypothesis, referred to as the Monro-Kellie Hypothesis (now better known as the Monro-Kellie Doctrine), states, “The sum of volumes of the brain, CSF, and intracranial blood is constant. An increase in one should cause a decrease in one or both of the remaining two.” Therefore, if an abundance of cerebrospinal fluid (IIH or hydrocephalus), both cranial blood volume and brain matter should be forced to deplete. This depletion is usually directed in the path of least resistance – through the foramen magnum and into the spinal canal. When the brain matter closest to the bottom of the skull (cerebellar tonsils) is pushed through the foramen magnum and into the spinal canal (an Acquired Chiari Malformation), the tonsils act like a cork and blocks the flow of cerebrospinal fluid (regardless of the size of the tonsillar descent), which in turn, continues to raise intracranial pressure.[3]

Venous Hypertension
When an etiological cofactor exists (such as a space-occupying mass), it is considered Secondary Intracranial Hypertension (SIH); when no other cause was identified, it is known as Idiopathic Intracranial Hypertension (IIH) formerly known as Pseudotumor Cerebri. However, recent studies on the connection between Intracranial Hypertension and Venous Hypertension might put an end to the “idiopathic” theory.
Oxygen-rich blood travels from the heart to the rest of the body through the arterial system, then the oxygen-depleted blood returns to the heart through the venous system. We have a host of small veins in our head and they dump into a series of large veins, called sinuses. Dural Venous Sinus Stenosis occurs when there is a narrowing of one or more of the venous sinuses (most commonly seen in the transverse sinuses or transverse/sigmoid sinus junction), which in turn compromises cerebral venous outflow through the jugular vein (stenosis/compression of the jugular vein can also result in elevated intracranial pressure [4]). Transverse Sinus Stenosis (TSS) is most common in Idiopathic Intracranial Hypertension (IIH). Depending on the study that you are reading, it is proving to be present in 90-100% of IIH patients [5]. While its connection might sound obscure if you look at it from a Monro-Kellie perspective – The blood going into the head, cannot get out at the same speed (because of the narrowed sinus). When this inflow of blood remains constant and the outflow is hindered, the transverse sinus on that side (we have two transverse sinuses, one on each side) enlarges, forcing the CSF and brain matter to reduce to maintain the volume equilibrium. This reciprocation can happen when any of the sinuses or jugular narrow (stenosis). While scholars continue to debate whether TSS is a cause or consequence of IIH, surgeons continue to decompress us without checking our pressures or decompress (the most invasive treatment) in hopes that it will lower our pressures, and patients are left with untreated high pressure still causing a “pushing down effect” and an enlarged foramen magnum for our brains to be pushed down. [2] The sagging brain once again obstructs the flow of cerebrospinal fluid by plugging the foramen magnum, and that in turn raises the intracranial pressure even more. Or, the untreated high pressure blows through the duraplasty and causes a post-operative leak, known as a pseudomeningocele.
Reducing the Risks of Post-Op IH/IIH Complications
Brain MRIs often show indicators of Intracranial Hypertension (IH/IIH), therefore, we recommend that all Chiari patients have full brain MRIs and not just cervical MRIs. 
• When the pressure builds inside of the dura mater the pressure pushes the dura and fluid inside of the crevice that holds the pituitary gland (the sella turcica or pituitary fossa). When the amount of fluid is equal to or greater than 50% and the pituitary gland size is 2mm, the condition is known as Empty Sella Syndrome. (Doctors now recognize that < 50% (where the pituitary gland size is 3-7mm) can also cause symptoms and they now refer to that as a partially empty sella.) [8]
• Slit like or flattened lateral ventricles from the increased pressure, however, when the Foramen of Monro (the aqueduct that connects the lateral ventricle to the third ventricle) is stenosed, the fluid will back-up and the lateral ventricle will not appear flattened. [7]
• Enlarged/swollen optical nerves (papilledema). [8]
• Low lying or herniated tonsils (often diagnosed as a Chiari Malformation). [2]
What We Recommend BEFORE DECOMPRESSION is considered:
If you have symptoms of IH/IIH accompanied by any of the MRI indicators mentioned above, it is both reasonable and prudent to ask your neurosurgeon to investigate further BEFORE DECOMPRESSION.
- See a neuro-ophthalmologist to check for signs of papilledema, including Optical Coherence Tomography and Ultrasonographic B-scanning. [8]
- Magnetic Resonance Venography (MRV, preferably with the ATECO technique) to check for venous stenosis of any of the cranial sinuses and/or jugular vein. Stenosis is not exclusive to the transverse sinus and it can happen in multiple sinuses simultaneously.
- If overweight, consider trying to lose weight. Studies show that a weight loss of 5-10% of one’s overall body weight, when accompanied by a low-salt diet, can offer some to IH/IIH symptoms.[9]
- Consider trying Diamox (Acetazolamide) and/or Topamax (Topiramate) to see if that improves the pressure headaches.
- Request a lumbar puncture (spinal tap) to test your opening pressures. We recommend that it’s guided with fluoroscopy with a small gauge needle (and not the standard 22 gauge) that they allow to drip (as opposed to syringe pull) and ensure that someone is available to perform an epidural blood patch if necessary. Time should be allotted afterward to lay flat for several hours immediately following the procedure and for several days once returning home. The potential for CSF leaks is high for the EDS/Chiari patient. A doctor that marginalizes the risks ahead of time, will generally marginalize your symptoms when you are actively leaking.
- ICP Bolt Monitoring can record the differences experienced in pressure over time, and how different positions affect ICP.
Note: When the intracranial pressure gets high enough, it can cause a cranial leak. This is especially true for the Ehlers-Danlos patient where the dura mater is thin and fragile. When a cranial leak decreases the intracranial pressure, the papilledema, empty sella, stenosis, and high-pressure headaches can sometimes start to revert to normal or near-normal, and the leak will affect any attempts to check intracranial pressure (reducing the pressure from what it was before the leak occurred), however, the tonsillar herniation will usually remain if the pressure gets too low. [10]
TREATMENT OPTIONS:
If Venous Stenosis exists, stenting should be considered as leaving the sinus/jugular stenosed can post other health risks, and stenting is proving to have much better success with fewer complications requiring revisions. When medication fails to decrease ICP, and a stent is not an option, a Ventriculoperitoneal Shunt (VP Shunt) or Ventriculoatrial Shunt (VA Shunt) can be surgically placed to drain cerebrospinal fluid straight from the ventricle. Shunts are known for failing and often need a multitude of revisions, but even with all the revisions, it is less invasive than a decompression. Shunts under the foramen magnum should never be used as a means of controlling ICP.
For the IH/IIH patient, herniated tonsils should be assumed an Acquired Chiari Malformation (even if a small posterior fossa is evident), and by correcting the high pressure before decompression, the decompression will be less likely to fail.
Helpful Tips:
If you have IH/IIH, it is best to avoid caffeine, avoid progestin based birth control, and all EDS patients should try to avoid the use of fluoroquinolones such as ciprofloxacin (Cipro), levofloxacin (Levaquin/Quixin), gatifloxacin (Tequin), moxifloxacin (Avelox), ofloxacin (Ocuflox/Floxin/Floxacin), norfloxacin (Noroxin), due to the increased risk of aneurysm.
[wpedon id=”4396″ align=”center”]
References:
1 Rangel-Castillo, Leonardo, et al. “Management of Intracranial Hypertension.” Rangel-Castilla, Leonardo et al. “Management of intracranial hypertension.” Neurologic clinics vol. 26,2 (2008): 521-41, x. doi:10.1016/j.ncl. Feb. 2008, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2452989/>.
2 Aiken, A.H., et al. “Incidence of Cerebellar Tonsillar Ectopia in Idiopathic Intracranial Hypertension: A Mimic of the Chiari I Malformation.” American Journal of Neuroradiology; Nov. 2012, <http://www.ajnr.org/content/33/10/1901>.
3 Mokri, B. “The Monro-Kellie Hypothesis: Applications in CSF Volume Depletion.” Neurology., U.S. National Library of Medicine, 26 June 2001, <https://www.ncbi.nlm.nih.gov/pubmed/11425944>.
4 Zhou, D., et al. “Intracranial hypertension induced by internal jugular vein stenosis can be resolved by stenting.” European Journal of Neurology, November 2017 <https://onlinelibrary.wiley.com/doi/abs/10.1111/ene.13512>.
5 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 21 Feb. 2017, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
6 Pietrangelo, Ann. “Empty Sella Syndrome.” Healthline, Oct. 2017, <https://www.healthline.com/health/empty-sella-syndrome>.
7 Hingwala, Divyata R., et al. “Imaging signs in idiopathic intracranial hypertension: Are these signs seen in secondary intracranial hypertension too?.” Annals of Indian Academy of Neurology vol. 16,2: 229-33. doi:10.4103/0972-2327.112476, June 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3724081/>.
8 Mollan, Susan P., et al. “A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertension.” Practical neurology vol. 14,6: 380-90. doi:10.1136/practneurol-2014-000821. May 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4251443/>.
9 Thurtell, Matthew J., and Michael Wall. “Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): Recognition, Treatment, and Ongoing Management.” Current Treatment Options in Neurology, U.S. National Library of Medicine, Feb. 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3554852/>.
10 Pérez, Mario A., et al. “Primary spontaneous cerebrospinal fluid leaks and idiopathic intracranial hypertension.” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4: 330-7. doi:10.1097/WNO.0b013e318299c292, Dec. 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>.


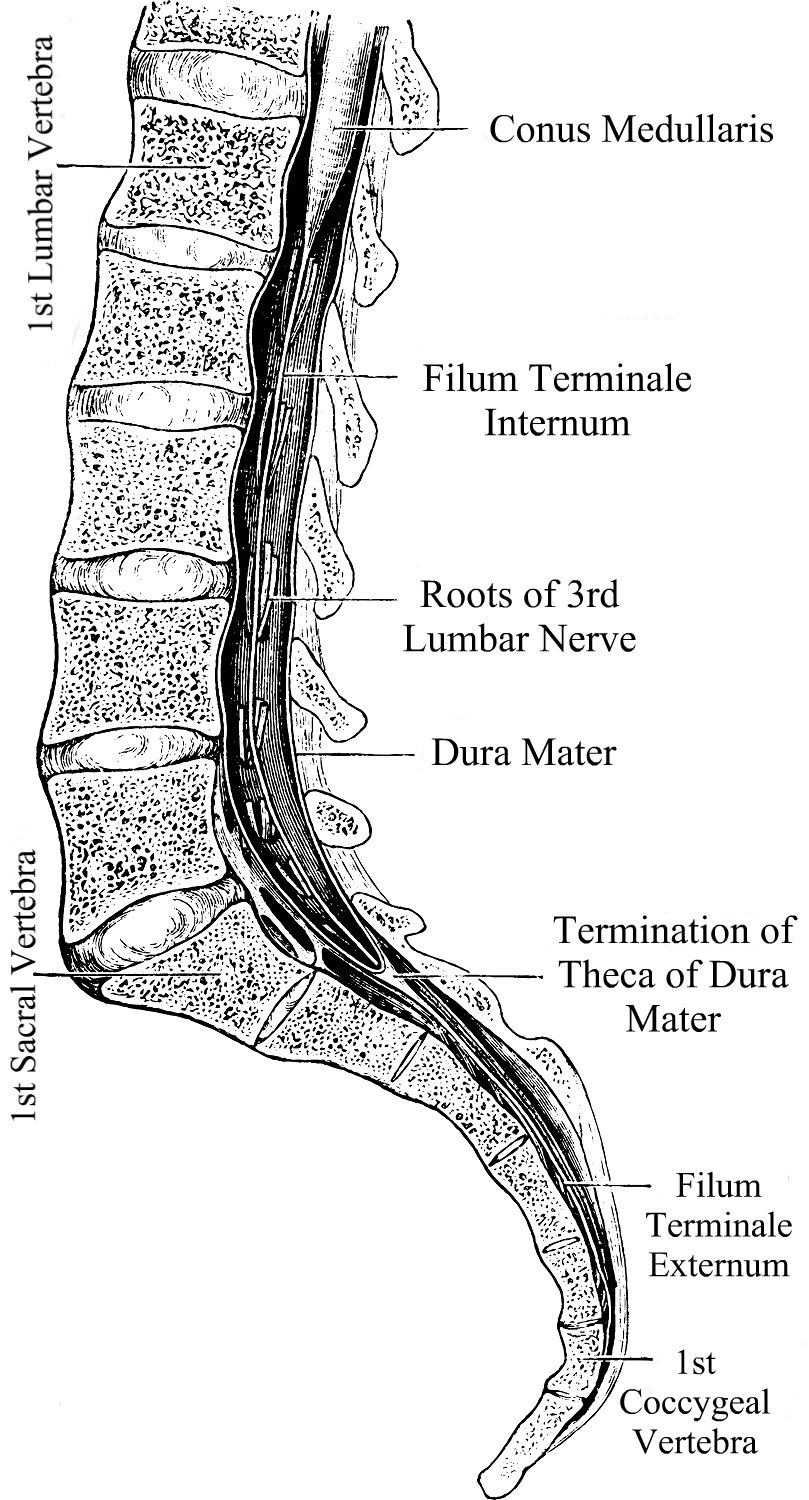
 Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.
Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.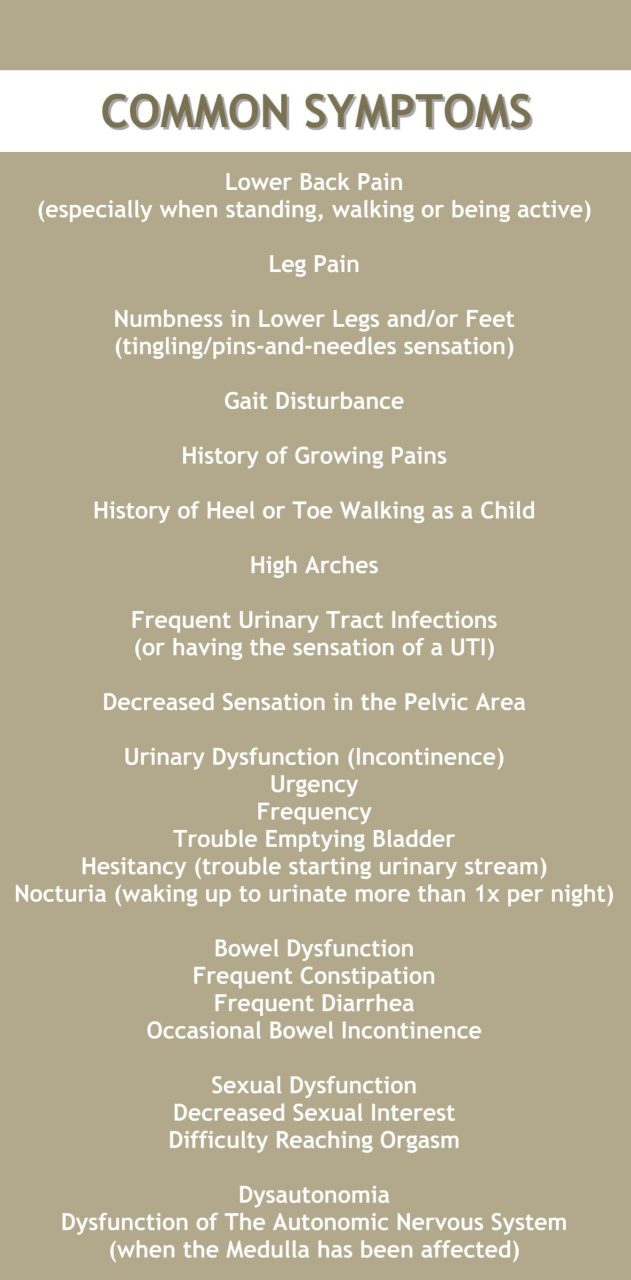
 What We Recommend
What We Recommend 

 When I first started getting hit with symptoms, I was a divorced, single mother of three amazing kids; responsible not only to provide for them but to see them through life, unscathed by life’s situations, and showing them that there was nothing that if they worked hard at something, nothing could hold them back. I had just started to expand in my career as a self-taught auto technician. I was a woman making a place for herself in an industry traditionally dominated by males. July 3, 2015, was the day that my life forever changed. I was brought to the hospital with stroke-like symptoms. I was having visual problems. I couldn’t walk or talk. I had no idea who I was or where I was. The whole right side of my body basically stopped working and the right side of my face was droopy. I was brought to the ER and before the doctor would even try to figure out what was wrong with me, he ordered a series of drug tests. I passed every test, so he finally admitted to me. Once on the neurology floor, more testing was done. They performed an MRI, MRA, EKG and told us that all results were normal. I later discovered that was not the case.
When I first started getting hit with symptoms, I was a divorced, single mother of three amazing kids; responsible not only to provide for them but to see them through life, unscathed by life’s situations, and showing them that there was nothing that if they worked hard at something, nothing could hold them back. I had just started to expand in my career as a self-taught auto technician. I was a woman making a place for herself in an industry traditionally dominated by males. July 3, 2015, was the day that my life forever changed. I was brought to the hospital with stroke-like symptoms. I was having visual problems. I couldn’t walk or talk. I had no idea who I was or where I was. The whole right side of my body basically stopped working and the right side of my face was droopy. I was brought to the ER and before the doctor would even try to figure out what was wrong with me, he ordered a series of drug tests. I passed every test, so he finally admitted to me. Once on the neurology floor, more testing was done. They performed an MRI, MRA, EKG and told us that all results were normal. I later discovered that was not the case. A few days later, I followed up with my PCP. She went over my MRI results with me and pointed out that they found a Chiari Malformation with a 19mm herniation of my cerebellar tonsils. She told me of changes in my white matter that the radiologist said needed to be “further evaluated” and referred me to my first neurologist, who I met within August. He ordered a visual evoked potential and an EEG. Both come back normal, so he diagnosed me with migraines, even after hearing my symptoms, which frustrates me even more as I know that it is not migraines causing these issues.
A few days later, I followed up with my PCP. She went over my MRI results with me and pointed out that they found a Chiari Malformation with a 19mm herniation of my cerebellar tonsils. She told me of changes in my white matter that the radiologist said needed to be “further evaluated” and referred me to my first neurologist, who I met within August. He ordered a visual evoked potential and an EEG. Both come back normal, so he diagnosed me with migraines, even after hearing my symptoms, which frustrates me even more as I know that it is not migraines causing these issues. During this care for MS, I kept having what they thought were MS relapses, roughly every three to four months. Each time they ordered new MRI images and treated me with high doses of IV steroids for five days in a row. Never once did this imaging ever show an actual MS-relapse or MS activity. I continually had issues with every medication that they put me on to help “try to delay the progression of the MS” (the MS that I never had). In November 2017 I started Ocrevus, which was just FDA approved that year. Around this time, I started having strange symptoms and thought them just to be side effects of the medication, not realizing that something else might be causing it all. I met with my neurologist before my second full dose and I told her everything that I was experiencing. We opted to take me off the Ocrevus and they repeated the MRI yet again. Again, the MRIs show absolutely nothing new for activity and she admits that she doesn’t know what to do for me. I am three years in at that point and never once have they seen any MS activity.
During this care for MS, I kept having what they thought were MS relapses, roughly every three to four months. Each time they ordered new MRI images and treated me with high doses of IV steroids for five days in a row. Never once did this imaging ever show an actual MS-relapse or MS activity. I continually had issues with every medication that they put me on to help “try to delay the progression of the MS” (the MS that I never had). In November 2017 I started Ocrevus, which was just FDA approved that year. Around this time, I started having strange symptoms and thought them just to be side effects of the medication, not realizing that something else might be causing it all. I met with my neurologist before my second full dose and I told her everything that I was experiencing. We opted to take me off the Ocrevus and they repeated the MRI yet again. Again, the MRIs show absolutely nothing new for activity and she admits that she doesn’t know what to do for me. I am three years in at that point and never once have they seen any MS activity. The last four years have been one hell of a ride when it comes to my health. My health problems have made it far more difficult to continue working on cars. As my symptoms wage war on my body, I am now forced to work on light duty and have been for the last two and a half years. I know that my days of working in a shop are coming to end as I just can’t handle the physical requirements of the job anymore. My quality of life in the last year alone has declined sharply. I used to be the energetic mom who could coach a sports team after working all day in the shop and still have the energy to keep up with the housework, now that is not the case. I manage to push on and get them to their activities, but I’m exhausted to the core. When this all began back in 2015 my kids were 8, 7, and 5. They are now 12, 11 and 9. At times I feel like I am a horrible mother because I miss the mom that I used to be. I miss the days when my kids weren’t worried about my health and when we could make plans with other families and keep them. I have lost so much of who I am thanks to the ignorance of some members of the medical community. I am losing faith in the medical profession in general. Male doctors have been the worst as I go through this journey, as women seem to have to first prove that it’s not psychosomatic before we’re worthy of being helped, even with imaging shows something to the contrary. When I present them with proven facts about Chiari Malformation, it still gets dismissed and it is extremely frustrating. The longer I go without receiving proper treatment, the more likely it becomes that some of this damage will become permanent and to me, that is not acceptable. I am fighting for my life and I will not back down until I receive the proper care, I can’t!
The last four years have been one hell of a ride when it comes to my health. My health problems have made it far more difficult to continue working on cars. As my symptoms wage war on my body, I am now forced to work on light duty and have been for the last two and a half years. I know that my days of working in a shop are coming to end as I just can’t handle the physical requirements of the job anymore. My quality of life in the last year alone has declined sharply. I used to be the energetic mom who could coach a sports team after working all day in the shop and still have the energy to keep up with the housework, now that is not the case. I manage to push on and get them to their activities, but I’m exhausted to the core. When this all began back in 2015 my kids were 8, 7, and 5. They are now 12, 11 and 9. At times I feel like I am a horrible mother because I miss the mom that I used to be. I miss the days when my kids weren’t worried about my health and when we could make plans with other families and keep them. I have lost so much of who I am thanks to the ignorance of some members of the medical community. I am losing faith in the medical profession in general. Male doctors have been the worst as I go through this journey, as women seem to have to first prove that it’s not psychosomatic before we’re worthy of being helped, even with imaging shows something to the contrary. When I present them with proven facts about Chiari Malformation, it still gets dismissed and it is extremely frustrating. The longer I go without receiving proper treatment, the more likely it becomes that some of this damage will become permanent and to me, that is not acceptable. I am fighting for my life and I will not back down until I receive the proper care, I can’t!
 Once diagnosed, you will usually be referred to a specialist (not a Chiari Specialist, but an everyday, run-of-the-mill neurologist or neurosurgeon). They tend to come in one of two types: Either they are very passive and just want to wait and see how bad it gets, or they are very pro-surgery and while they will still usually give you a 50% chance of helping your symptoms, they will tell you how decompression surgery really is your best option. Both are problematic.
Once diagnosed, you will usually be referred to a specialist (not a Chiari Specialist, but an everyday, run-of-the-mill neurologist or neurosurgeon). They tend to come in one of two types: Either they are very passive and just want to wait and see how bad it gets, or they are very pro-surgery and while they will still usually give you a 50% chance of helping your symptoms, they will tell you how decompression surgery really is your best option. Both are problematic.