Most Chiarians go to see a surgeon with an expectation of them being knowledgeable in their field. However, while they might be a neurosurgeon, their knowledge of Chiari and its comorbid/pathological conditions might not rank high in their practice. Make the most of your initial appointment by interviewing them and what they really know about Chiari Malformations. Be cautious of inflated success rates. Chiari decompression in general offers a just over a 50% success rate (which means it has a nearly 50% failure rate). Surgeons that claim a 100% (or near 100% success rate) are usually not basing their success on how their patients feel afterward, it is based on if they were successful with the aspects of the surgery: Removal of the occipital bone ✓ Opening the dura and adding the patch/graft ✓ Laminectomy ✓ Cauterization/resection of cerebellar tonsils ✓
WE DESERVE BETTER THAN THAT!
HERE IS A LIST OF CHIARI QUESTIONS WE RECOMMEND ASKING AT YOUR FIRST NEUROSURGERY APPOINTMENT:
General Questions:
How do you define a Chiari Malformation?
What do you believe causes a Chiari malformation?
Are all Chiari malformations from a small posterior fossa?
Do I have a small posterior fossa? If yes, how big is it? If size is unknown, was my posterior fossa measured? If not, why not? How did you come to the conclusion that I have a small posterior fossa?
How common do you believe Acquired Chiari malformations to be?
Do you always recommend decompression surgery for all of your patients with herniated cerebellar tonsils? Why/why not?
In an average month, how many Chiari decompressions do you perform? How many tethered cord releases? How many craniocervical fusions? What percentage of your practice is spent treating patients with these connective tissue related conditions?
Looking at my brain scan, is any part of my “brainstem” herniated (below the posterior fossa)? If so, does that make me a Chiari 1.5?
Intracranial Hypotension (low pressure) Questions: *Article to help you understand CSF Leaks & Intracranial Hypotension prior to your appointment. If you have SYMPTOMS OF LOW INTRACRANIAL PRESSURE and/or suspect a cerebrospinal fluid leak, we recommend asking the following questions:
S.E.E.P.S.
Looking at my brain scan, do you see any Subdural fluid collections?
Looking at my brain scan, do you see an Enhancement of pachymeninges?
Looking at my brain scan, do you see an Engorgement of my venous structures? Should we do an MRV to make sure?
Looking at my brain scan, does my Pituitary appear to be enlarged?
Looking at my brain scan, does my brain appear to be Sagging?
Looking at my corpus callosum:
Does there appear to be a depression?
Is there an inferior pointing of the splenium?
If he/she answers affirmatively to any of the above S.E.E.P.S. questions, ask:
What should be done to find/repair a potential leak?
Are you aware that it is common for CSF Leaks to not show up on MRI?
Are you willing to do a CT Myelogram and/or a digital subtraction myelogram, if I develop symptoms of a leak and none can be found on MRI?
Are you aware that it can often take multiple epidural blood patches to try and seal a leak, and sometimes when a blood patch fails to work, a surgical dural repair might be necessary?
Intracranial Hypertension (high pressure) Questions: *Article to help you understand Intracranial Hypertension prior to your appointment. If you have SYMPTOMS OF HIGH INTRACRANIAL PRESSURE, we recommend asking the following questions:
Looking at my brain scan, do I have cerebrospinal fluid in my sella turcica (Empty Sella Syndrome)?
Looking at my brain scan, do you see any evidence of my optic nerves are swollen (papilledema)?
If so, should I be referred to a neuro-ophthalmologist?
Looking at my brain scan, do my lateral ventricles appear small or flattened?
If so, do I need to have my pressures checked?
If yes, are you aware of the risks of developing a CSF Leak from a lumbar puncture?
What are the symptoms of a CSF Leak, should one develop?
What is your plan of action if I should develop these leak symptoms?
Are you aware that it is common for CSF Leaks to not show up on MRI?
Are you willing to do a CT Myelogram if I develop symptoms of a leak, and none can be found on MRI?
Should a leak be found, are you aware that it can often take multiple epidural blood patches to try and seal a leak?
Tethered Cord Questions: *Article to help you understand Tethered Cord: Sorry, Coming Soon. If you have SYMPTOMS OF TETHERED CORD, we recommend asking the following questions:
Looking at my brain/cervical scan, does my brainstem appear to be elongated?
Looking at my cervical scan, does my spinal cord appear to be stretched?
Looking at my lumbar scan, does my conus reach my mid/low L2?
Looking at my thoracic and lumbar scan, does my spinal cord appear to be pulling to the back, or one particular side?
If so, should we do a prone MRI to see if it has actually adhered to that side?
Looking at my lumbar scan, do I appear to have fatty tissue inside the epidermis?
If the answer to any of these questions is affirmative, do you suspect that I have a tethered spinal cord?
If so, should we plan for a Tethered Cord Release before or soon after decompression surgery, so the likelihood of a failed decompression is reduced?
If I have urological issues, can I get a referral for urodynamic testing to rule out any other potential causes of my urological issues?
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI): *Article to help you understand CCI & AAI prior to your appointment. If you have SYMPTOMS OF CRANIOCERVICAL INSTABILITY or SYMPTOMS OF ATLANTOAXIAL INSTABILITY, we recommend asking the following questions:
Looking at my brain/cervical scans, what are the measurements of my clivoaxial angle and Grabb-Oakes?
Do these measurements meet the diagnostic criteria for Craniocervical Instability?
Looking at my flexion and extension imaging, how many millimeters of translation are there between flexion and extension?
Does Chamberlain’s Line cross my odontoid? If so, does it cross at a level that would indicate Basilar Invagination?
Looking at my rotational imaging, what is the percentage of uncovering of the right and left articular facets on rotation?
Do the percentages from my rotational imaging meet the diagnosis criteria for Atlantoaxial Instability?
IF A DIAGNOSIS CRITERIA IS MET IN ANY OF THE ABOVE, WE STRONGLY RECOMMEND THAT YOU WAIT ON DECOMPRESSION AND PURSUE THE TREATMENT OF SAID CONDITION(S) AND THAT OF EHLERS-DANLOS SYNDROME, AS EACH OF THESE CONDITIONS CAN BE PATHOLOGICAL TO AN ACQUIRED CHIARI AND EACH IS A STRONG INDICATOR THAT A CONNECTIVE TISSUE PROBLEM EXISTS.
*The questions in this article will periodically change as we are able to expand our recommended questions.
*Original version released September 2018, revised 2023.
INTRACRANIAL HYPERTENSION (IH) MEANS HIGH PRESSURE INSIDE THE SKULL.
Intracranial Pressure (ICP) is measured in millimeters of mercury (mmHg). Most scholars agree that on average, “normal pressure” should be between 5-15 mmHg, mild to moderate intracranial hypertension between 20-30 mmHg (which “requires treatment in most circumstances”), and an ICP of > 40 mmHg indicates “severe and possibly life-threatening intracranial hypertension.” [1] When high intracranial pressure is left untreated, it creates a “pushing effect” towards the only natural escape at the base of the skull (the foramen magnum), and the cerebellar tonsils in the pathway are pushed through the foramen magnum. [2]
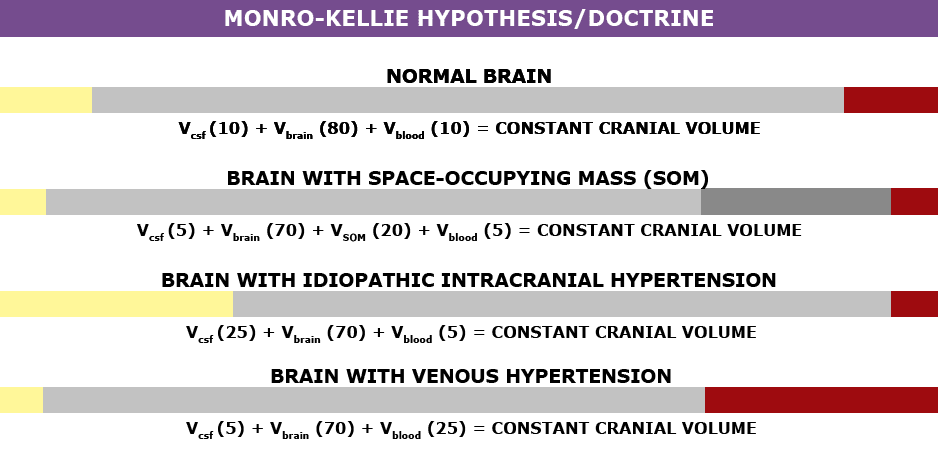
Understanding the Monro-Kellie Doctrine (pressure-volume relationship) The association between IH/IIH and Chiari Malformation appears to be a malicious intricate pathological circle. The cranium (skull) consists of brain matter, cerebrospinal fluid, and both venous and arterial blood. A hypothesis, referred to as the Monro-Kellie Hypothesis (now better known as the Monro-Kellie Doctrine), states, “The sum of volumes of the brain, CSF, and intracranial blood is constant. An increase in one should cause a decrease in one or both of the remaining two.” Therefore, if an abundance of cerebrospinal fluid (IIH or hydrocephalus), both cranial blood volume and brain matter should be forced to deplete. This depletion is usually directed in the path of least resistance – through the foramen magnum and into the spinal canal. When the brain matter closest to the bottom of the skull (cerebellar tonsils) is pushed through the foramen magnum and into the spinal canal (an Acquired Chiari Malformation), the tonsils act like a cork and blocks the flow of cerebrospinal fluid (regardless of the size of the tonsillar descent), which in turn, continues to raise intracranial pressure.[3]
Venous Hypertension
When an etiological cofactor exists (such as a space-occupying mass), it is considered Secondary Intracranial Hypertension (SIH); when no other cause was identified, it is known as Idiopathic Intracranial Hypertension (IIH) formerly known as Pseudotumor Cerebri. However, recent studies on the connection between Intracranial Hypertension and Venous Hypertension might put an end to the “idiopathic” theory.
Oxygen-rich blood travels from the heart to the rest of the body through the arterial system, then the oxygen-depleted blood returns to the heart through the venous system. We have a host of small veins in our head and they dump into a series of large veins, called sinuses. Dural Venous Sinus Stenosis occurs when there is a narrowing of one or more of the venous sinuses (most commonly seen in the transverse sinuses or transverse/sigmoid sinus junction), which in turn compromises cerebral venous outflow through the jugular vein (stenosis/compression of the jugular vein can also result in elevated intracranial pressure [4]). Transverse Sinus Stenosis (TSS) is most common in Idiopathic Intracranial Hypertension (IIH). Depending on the study that you are reading, it is proving to be present in 90-100% of IIH patients [5]. While its connection might sound obscure if you look at it from a Monro-Kellie perspective – The blood going into the head, cannot get out at the same speed (because of the narrowed sinus). When this inflow of blood remains constant and the outflow is hindered, the transverse sinus on that side (we have two transverse sinuses, one on each side) enlarges, forcing the CSF and brain matter to reduce to maintain the volume equilibrium. This reciprocation can happen when any of the sinuses or jugular narrow (stenosis). While scholars continue to debate whether TSS is a cause or consequence of IIH, surgeons continue to decompress us without checking our pressures or decompress (the most invasive treatment) in hopes that it will lower our pressures, and patients are left with untreated high pressure still causing a “pushing down effect” and an enlarged foramen magnum for our brains to be pushed down. [2] The sagging brain once again obstructs the flow of cerebrospinal fluid by plugging the foramen magnum, and that in turn raises the intracranial pressure even more. Or, the untreated high pressure blows through the duraplasty and causes a post-operative leak, known as a pseudomeningocele.
Reducing the Risks of Post-Op IH/IIH Complications
Brain MRIs often show indicators of Intracranial Hypertension (IH/IIH), therefore, we recommend that all Chiari patients have full brain MRIs and not just cervical MRIs.
• When the pressure builds inside of the dura mater the pressure pushes the dura and fluid inside of the crevice that holds the pituitary gland (the sella turcica or pituitary fossa). When the amount of fluid is equal to or greater than 50% and the pituitary gland size is 2mm, the condition is known as Empty Sella Syndrome. (Doctors now recognize that < 50% (where the pituitary gland size is 3-7mm) can also cause symptoms and they now refer to that as a partially empty sella.) [8]
• Slit like or flattened lateral ventricles from the increased pressure, however, when the Foramen of Monro (the aqueduct that connects the lateral ventricle to the third ventricle) is stenosed, the fluid will back-up and the lateral ventricle will not appear flattened. [7]
• Low lying or herniated tonsils (often diagnosed as a Chiari Malformation). [2]
What We Recommend BEFORE DECOMPRESSION is considered:
If you have symptoms of IH/IIH accompanied by any of the MRI indicators mentioned above, it is both reasonable and prudent to ask your neurosurgeon to investigate further BEFORE DECOMPRESSION.
See a neuro-ophthalmologist to check for signs of papilledema, including Optical Coherence Tomography and Ultrasonographic B-scanning. [8]
Magnetic Resonance Venography (MRV, preferably with the ATECO technique) to check for venous stenosis of any of the cranial sinuses and/or jugular vein. Stenosis is not exclusive to the transverse sinus and it can happen in multiple sinuses simultaneously.
If overweight, consider trying to lose weight. Studies show that a weight loss of 5-10% of one’s overall body weight, when accompanied by a low-salt diet, can offer some to IH/IIH symptoms.[9]
Consider trying Diamox (Acetazolamide) and/or Topamax (Topiramate) to see if that improves the pressure headaches.
Request a lumbar puncture (spinal tap) to test your opening pressures. We recommend that it’s guided with fluoroscopy with a small gauge needle (and not the standard 22 gauge) that they allow to drip (as opposed to syringe pull) and ensure that someone is available to perform an epidural blood patch if necessary. Time should be allotted afterward to lay flat for several hours immediately following the procedure and for several days once returning home. The potential for CSF leaks is high for the EDS/Chiari patient. A doctor that marginalizes the risks ahead of time, will generally marginalize your symptoms when you are actively leaking.
ICP Bolt Monitoring can record the differences experienced in pressure over time, and how different positions affect ICP.
Note: When the intracranial pressure gets high enough, it can cause a cranial leak. This is especially true for the Ehlers-Danlos patient where the dura mater is thin and fragile. When a cranial leak decreases the intracranial pressure, the papilledema, empty sella, stenosis, and high-pressure headaches can sometimes start to revert to normal or near-normal, and the leak will affect any attempts to check intracranial pressure (reducing the pressure from what it was before the leak occurred), however, the tonsillar herniation will usually remain if the pressure gets too low. [10]
TREATMENT OPTIONS:
If Venous Stenosis exists, stenting should be considered as leaving the sinus/jugular stenosed can post other health risks, and stenting is proving to have much better success with fewer complications requiring revisions. When medication fails to decrease ICP, and a stent is not an option, a Ventriculoperitoneal Shunt (VP Shunt) or Ventriculoatrial Shunt (VA Shunt) can be surgically placed to drain cerebrospinal fluid straight from the ventricle. Shunts are known for failing and often need a multitude of revisions, but even with all the revisions, it is less invasive than a decompression. Shunts under the foramen magnum should never be used as a means of controlling ICP.
For the IH/IIH patient, herniated tonsils should be assumed an Acquired Chiari Malformation (even if a small posterior fossa is evident), and by correcting the high pressure before decompression, the decompression will be less likely to fail.
Helpful Tips: If you have IH/IIH, it is best to avoid caffeine, avoid progestin based birth control, and all EDS patients should try to avoid the use of fluoroquinolones such as ciprofloxacin (Cipro), levofloxacin (Levaquin/Quixin), gatifloxacin (Tequin), moxifloxacin (Avelox), ofloxacin (Ocuflox/Floxin/Floxacin), norfloxacin (Noroxin), due to the increased risk of aneurysm.
[wpedon id=”4396″ align=”center”]
References:
1 Rangel-Castillo, Leonardo, et al. “Management of Intracranial Hypertension.” Rangel-Castilla, Leonardo et al. “Management of intracranial hypertension.” Neurologic clinics vol. 26,2 (2008): 521-41, x. doi:10.1016/j.ncl. Feb. 2008, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2452989/>.
2 Aiken, A.H., et al. “Incidence of Cerebellar Tonsillar Ectopia in Idiopathic Intracranial Hypertension: A Mimic of the Chiari I Malformation.” American Journal of Neuroradiology; Nov. 2012, <http://www.ajnr.org/content/33/10/1901>.
3 Mokri, B. “The Monro-Kellie Hypothesis: Applications in CSF Volume Depletion.” Neurology., U.S. National Library of Medicine, 26 June 2001, <https://www.ncbi.nlm.nih.gov/pubmed/11425944>.
5 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 21 Feb. 2017, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
7 Hingwala, Divyata R., et al. “Imaging signs in idiopathic intracranial hypertension: Are these signs seen in secondary intracranial hypertension too?.” Annals of Indian Academy of Neurology vol. 16,2: 229-33. doi:10.4103/0972-2327.112476, June 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3724081/>.
8 Mollan, Susan P., et al. “A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertension.” Practical neurology vol. 14,6: 380-90. doi:10.1136/practneurol-2014-000821. May 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4251443/>.
9 Thurtell, Matthew J., and Michael Wall. “Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): Recognition, Treatment, and Ongoing Management.” Current Treatment Options in Neurology, U.S. National Library of Medicine, Feb. 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3554852/>.
10 Pérez, Mario A., et al. “Primary spontaneous cerebrospinal fluid leaks and idiopathic intracranial hypertension.” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4: 330-7. doi:10.1097/WNO.0b013e318299c292, Dec. 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>.
When you start to educate yourself on a condition like Chiari, your vocabulary will be challenged. Most of us study with a medical journal article opened in one tab and medical dictionary in the next. Amongst all the medical terminology you will tackle, there are probably a few terms as important to your understanding of Chiari than comorbidities and pathological/etiological cofactors. When two or more conditions tend to co-occur, they are said to be comorbid with one another. It makes no inferences of a causal relationship between the conditions, only that they co-occur. This co-occurrence deduces that a correlation exists, but when the nature of that correlation is not known, they are just said to be comorbidities. When a “causal relationship” is known or suspected, the conditions start being discussed in terms of pathology or etiology, which are similar, but not exactly the same thing.
An etiological cofactor exists when the “root cause” of a condition is known or believed to be known. That “root cause” is the etiological cofactor. When an etiological cofactor can cause a series of events or conditions that can become “direct causes” for other conditions, that series of events creates a pathology. Conditions along the path are called pathological cofactors. Understanding these cofactors is imperative in understanding Chiari and all of the comorbid conditions that accompany it.
ETIOLOGICAL COFACTOR:
Chiari Malformation often seems like a beast that wreaks havoc on our bodies on every level. Indeed it is, but as you can see from the diagram above, it really is not the “root” of everything that is going wrong. There is a bigger beast at work in so many of us, and its name is Ehlers-Danlos. It is not by chance that so many of us with Chiari have so many other conditions in common (especially conditions like Degenerative Disc Disease, arthritis and other connective tissue problems). It is not by chance that so many of us have a history of miscarriage and similar familial histories. It is not by chance that Chiari is more prevalent in females than males. And it is definitely not by chance that Chiari is running in families and they cannot find a definitive genetic link. They cannot find it because they are not looking at the beast hiding in the background.
Ehlers-Danlos Syndromes are a group of inherited disorders involving a genetic mutation in one or more of our bodies’ collagen. Collagen is the most abundant protein, making up 1/3 of the proteins in the human body, affecting our bones, skin, muscles, and connective tissue[1]. Collagen is often described as a “cellular glue” that helps hold the body together. When that glue fails to hold, everything seems to go awry; before and after birth: skulls can under-develop in utero, organs tend to prolapse, and bones begin to shift as joint laxity increases (including the bones/vertebrae at the craniocervical junction). Ehlers-Danlos is a primary “root cause” of Chiari Malformations and a majority of the other problems we have. The list in blue is far from being a complete list of conditions caused by EDS. They are commonly accompanied with Chiari because they can cause or attribute to a Chiari malformation (pathological cofactors).[2]
PATHOLOGICAL COFACTORS:
Cranial Settling occurs when the skull has dropped and the odontoid (C2/axis) enters into the foramen magnum (Basilar Invagination). This drop can further compromise the craniocervical junction and as it pushes everything down, it increases the likelihood of an Acquired Chiari Malformation.
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI) usually occurs with cranial settling and Basilar Invagination (BI). The settling and/or softening of tissue can cause a shifting of the C2 (resulting in CCI or AAI) and the cerebellar tonsils (which are already inclined to prolapse) simply drop down with each shift affecting ones ability to tilt/rotate their head.[3]
Intracranial Hypertension (IH – High Intracranial Pressure) occurs when your intracranial pressure (ICP) becomes elevated. This elevation can happen for a variety of reasons.
Space Occupying Masses (cysts, tumors or hydrocephalus) take up space inside the skull causing a “mass effect.”
When no mass effect exists, many doctors look no further and give the diagnosis of Idiopathic Intracranial Hypertension.
Because the area of the skull is fixed in an adult cranium and partially fixed in that of a child, the elements inside the fixed space (CSF, blood volume and brain matter) tend to get pushed out wherever they can (the only place that they can escape without breaking through the dura is through the foramen magnum and the brain matter that’s closest to the foramen magnum is the cerebellar tonsils).[4]
Tethered Cord Syndrome occurs when the tissue inside the epidermis adheres to the spinal cord or filum terminale. While this tethering can happen anywhere along the spinal canal, it is most common in the lower lumbar and/or sacral spine. When this adhesion happens it creates a pulling down of the spinal cord and consequently, the brainstem located at the top of the spinal cord and the cerebellar tonsils just get pulled down with it.[5]
Intracranial Hypotension (Low Intracranial Pressure, often involving a CSF Leak) usually involves a cerebrospinal fluid leak or an over-draining shunt, we will highlight the former. Ehlers-Danlos patients tend to have weak dura matter. Tears/holes in the dura can happen anywhere in the dura surrounding the brain or spinal canal and they can happen completely spontaneously (without a known cause). When the leak occurs in the spinal canal, they can create a suctioning effect where cerebrospinal fluid (CSF) is being pulled down and out, causing the intracranial pressure (ICP) to drop. The cerebellar tonsils that are already prone to prolapse (due to EDS) end up getting suctioned downward with the CSF.[6] Cranial leaks often happen when high pressure is left untreated until the high pressure causes a leak in the dura mater. In cranial leaks, fluid usually leaks through the nose or ears (less common), and you can often taste the metallic taste of the cerebrospinal fluid in the back of your throat. While both spinal leaks and cranial leaks can cause low pressure and low-pressure symptoms, and while both can start, stop, and start again spontaneously, there is an increased risk whenever there is an opening where cerebrospinal fluid leaks outside of the human body (if cerebrospinal fluid can make it out of the body, microscopic bacteria can make it inside the same opening where it can enter in the meninges).[7]
Posterior Cranial Fossa Hypoplasia (PCFH) is the only etiological cofactor listed above that is definitely congenital. The role of collagen in bone development has been long-standing, especially its known contribution to certain conditions like Osteogenesis Imperfecta. However, more recent studies are discovering the role collagen plays in congenital posterior fossa anomalies. Posterior Cranial Fossa Hypoplasia is the most commonly “acclaimed” cause of Chiari malformations, but studies show, that even when all of the other causes above are factored out, only approximately 52% of those left (that fail to meet “the diagnosis criteria” for any of the above), have a small posterior fossa.[8]
COMORBIDITIES:
While all of the conditions listed in the diagram are comorbidities, some are etiological/pathological of an Acquired Chiari (even though nearly 100% of us are told that our Chiari Malformation is congenital) and others have Chiari Malformation as their etiological/pathological cofactor:
Syringomyelia occurs when cerebrospinal fluid (CSF) is obstructed and a CSF filled cyst/cavity forms inside the spinal cord. This cyst is directly related to the obstruction of cerebrospinal fluid that can be caused by Chiari Malformation, Spinal Stenosis (a narrowing of the spinal canal, spinal cyst/tumor, a herniated disc), or irregular curvature of the spine (scoliosis). When that cyst/cavity extends into the medulla oblongata (the lowest part of the brainstem), it is called Syringobulbia, and it comes with a new set of symptoms consistent with the damage being done to the brainstem. So when Chiari Malformation exists with a syrinx, and there is no stenosis or disc problem in close proximity below it, the Chiari Malformation should be listed as the etiological condition of the syrinx. If more than just the Chiari Malformation is believed to be causing the syrinx, each would be more accurately described as pathological.
Dysautonomia occurs when damage has been done to the brainstem or Vagus nerve. Whenever either of these is damaged, often from compression at/near the craniocervical junction, the autonomic nervous system can begin to dysfunction.
Confused? If you understand the causal relationships but find yourself wondering if a comorbid condition is an etiological or a pathological, think of it in terms of a domino effect. Only the first domino is etiological. All of the dominoes in between (on the path) are pathological. The important thing to remember in this array of medical terminology is that while everything is definitely not Chiari, it almost always shares a connection to it, and that is why so many of us have so many conditions and symptoms that doctors call unrelated! It is imperative in our fight that we know “what” we have and “why” it is happening. With such a broad spectrum of symptoms (like we all have), we must educate ourselves and not just believe the limited knowledge of our doctors.
7 Pérez, Mario A et al. “Primary Spontaneous Cerebrospinal Fluid Leaks and Idiopathic Intracranial Hypertension” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4 (2013): 330-7. doi:10.1097/WNO.0b013e318299c292, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>
THE DEFINITION OF A CHIARI MALFORMATION HAS BEEN LONG DEBATED. IT REALLY IS NO WONDER THAT PATIENTS AND MEDICAL PROFESSIONALS ALIKE ARE CONFUSED. THEN, WITH US FULLY UNDERSTANDING ALL SIDES OF THE DEBATE, WE DEFINED A CHIARI MALFORMATION AS STRUCTURAL DEFECTS IN WHICH THE CEREBELLUM, THE HIND PART OF THE BRAIN, DESCENDS BELOW THE FORAMEN MAGNUM INTO THE SPINAL CANAL. THIS DEBATE IS BEING ANALYZED THIS YEAR, AS CERTAIN ORGANIZATIONS ARE BRAVING TO ATTEMPT TO BRING DOCTORS ALL UNDER ONE UNIFORM DEFINITION AND DIAGNOSTIC CRITERIA. THEREFORE, AMIDST ALL THE CONFUSION AND DEBATE, WE WANTED TO EXPLAIN THE FACTORS INVOLVED, AND WHY WE WENT WITH THE DEFINITION THAT WE DID, AND WHY ONE STANDARD IS SO IMPORTANT!
To better facilitate our explanation, we will call all associated terms by their specific medical names:
Tonsillar Ectopia (TE) = tonsillar herniation of any size Posterior Fossa Hypoplasia (PFH) = an underdeveloped posterior fossa
Chiari Malformation Vs. Arnold Chiari Malformation
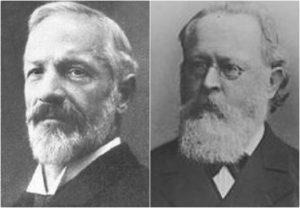
The most common type of Chiari is Type 1 (which includes a Chiari 1.5, where the brainstem is also below the foramen magnum). Many people use the term “Chiari Malformation” when diagnosed with Type 1, while others cling to the name “Arnold Chiari Malformation” with the same diagnosis. Is there a difference? The name “Chiari Malformation” came from Hans Chiari, an Austrian pathologist, who first discovered the malformation in the late 19th century.[1, 2] Julius Arnold, a German pathologist, later expanded on Chiari Type 2, and Type 2 took on his name “Arnold Chiari Malformation.” Therefore, technically speaking, a Chiari Malformation and an Arnold Chiari Malformation are not the same; Arnold Chiari Malformation is specific to Chiari Type 2 (which usually includes a myelomeningocele, the most serious form of Spina Bifida). However, they are used interchangeably by many, even by medical professionals and the misnomer is of little consequence one way or the other.[3]
Chiari Malformation = Posterior Fossa Hypoplasia Theory
Many ascribe to the theory that a Chiari Malformation ONLY consists of a posterior fossa hypoplasia (which means that the back of the skull is malformed, and therefore the cranial area (space) at the rear is too small). They believe that a tonsillar ectopia is only a symptom, and a Chiari Malformation can exist with or without an accompanying ectopia. This argument is not without merit, because much of what was initially being looked at by Hans Chiari were deformities in the posterior skull upon postmortem examination (so there wasn’t soft tissue to analyze). He originally attributed much to hydrocephalus, but expanded his research into the pons, medulla oblongata, and cerebellum (which can all be attributed to intracranial pressure as a pathology of a “tonsillar ectopia”). To ascribe to this belief would also mean that “Acquired Chiari Malformations” cannot exist, as one doesn’t “acquire” a small posterior fossa. And that would also mean that Chiari Type 2, Type 3 and Type 4 technically would not be a Chiari Malformation at all either, since their definitions do not require a posterior fossa hypoplasia. Perhaps type 3, which has an opening at the back of the skull, but no “small posterior fossa” is even implied in the definitions.
But to look at the full history of what became known as a Chiari Malformation, we can begin by looking at the research of a German pathologist, named Theodor Langhans. In his research in 1881 (a decade before Hans Chiari conducted his research on what became known as a Chiari Malformation), while looking at syringomyelia (“a cavity created in the spinal cord”), he noted a “change in the cerebellar cavity.” Upon dissection of the cerebellum, he described the cerebellar tonsils as “two symmetrical pyramidal tumors,” pushing the brainstem forward.[4] In fact, the other noted researchers: Nicholas Tulp (1593–1674), John Cleland (1835–1925), and Julius Arnold (1835–1915), all centered on the hindbrain hernia [herniation] without speculation as to its etiology/pathology. It is said that “many of the English translations of Chiari’s work contain inaccuracies.” But note that Chiari’s first paper was on “ectopia of cerebellar tissue,” and that he went on to define Type 1 as showing, “elongation of the tonsils and medial parts of the inferior lobes of the cerebellum into cone shaped projections, which accompany the medulla oblongata into the spinal canal.”[5] Which sounds like what is now known to be a Chiari 1.5. Much later, in 1938, at a time when the posterior fossa decompression became the popular surgical treatment for a Chiari Malformation, a Chiari 2 patient “underwent posterior fossa exploration with the authors not considering hindbrain herniation in their differential. Penfield and Coburn later stated that: ‘In retrospect it seems that we should have suspected the Arnold-Chiari malformation. Instead, a suboccipital craniotomy was carried out…” So even the early neurosurgeons seeking to perfect their surgical treatment felt that it was a mistake to concentrate on the posterior fossa and not take into account etiologies of the hindbrain herniation. That mistake is still going on 80 years later.[6]
The biggest problem that they are going to have with strictly defining a Chiari Malformation as a small posterior fossa resides in the fact that the diagnosis criteria for a Chiari Malformation only consists of ONE MEASUREMENT, the length of the tonsillar ectopia (how far the tonsils herniate below the foramen magnum). Generally, there are no measurements of the posterior fossa taken when radiologists make the initial diagnoses. Furthermore, most neurosurgeons see the radiology reports, and depending on symptomology, they make the decision to decompress or not to decompress without ever measuring the size of the posterior fossa. Most never look for (and often do not know about) etiological/pathological cofactors that could have been causing the tonsillar prolapse in the first place.
Where does this assumption leave us?
Unfortunately it leaves most of us with failed decompressions, fighting with our neurosurgeons that “something is still wrong.” These neurosurgeons look at their post-operative checklist and see that they successfully did everything surgically required in their out-of-date textbooks:
Suboccipital bone was appropriately decompressed. ✔️
Dura was opened and dura patch was successfully inserted. ✔️
Lamina was successfully removed from the C1 (and sometimes the C2 as well). ✔️
They did all that was required of them based on the diagnoses presented! They don’t have time (or don’t care) to look beyond that, so once again, the idea of our continued symptoms are thought of as being psychosomatic.
While we applaud the efforts of those seeking to get a measure of consistency in how Chiari is defined, the truth remains that until the diagnosis criteria is changed as well, we are being diagnosed with Chiari Malformation based on our tonsillar herniation; it is presumed to be congenital; we are being surgically treated as though it is congenital, and we are ending up with failed decompressions. This confusion is beyond unacceptable, it’s reprehensible!
When it is all redefined, hopefully we will have a well defined diagnosis criteria, or it is all irrelevant. And the many that really did acquire what was assumed to be “congenital” who are now being told that they do not have Chiari Malformation at all, will be able to get lawyers for “an improper diagnosis” that lead to the incorrect brain surgery being done. There are surgeons coming around and finally seeing that there is merit to these studies that have been done since the late 1990s, that have shown a pushing/pulling effect that can cause the tonsillar ectopia that gets us diagnosed with a Chiari Malformation, and we applaud them for having the integrity to stand up and get it right. That’s exactly what we need and deserve!
If you were diagnosed with a Chiari Malformation and want to know how all of this might be affecting you, we encourage you first to find your initial radiology reports, and see if there were measurements taken of the posterior fossa. And then wait with that information… wait and see what changes are actually made to the definition. While you are waiting learn. Learn everything you can about every etiological/pathological cofactor, and every comorbidity. If it is “officially” redefined as a small posterior fossa, we will have to work together as a community (like we always do) to help lawyers see how we have been getting lost in the shuffle, year after year. If it’s not officially changed and Chiari continues to be defined as a structural defect involving the cerebellar tonsils, we will have to continue in our fight to make these cofactors of Acquired Chiari Malformation known!
4 Mortazavi, M M, et al. “The First Description of Chiari I Malformation with Intuitive Correlation between Tonsillar Ectopia and Syringomyelia.” Advances in Pediatrics., U.S. National Library of Medicine, Mar. 2011, <https://www.ncbi.nlm.nih.gov/pubmed/21361763>.
5 Pearce, J M S. “Arnold Chiari, or ‘Cruveilhier Cleland Chiari’ Malformation.” Journal of Neurology, Neurosurgery & Psychiatry, BMJ Publishing Group Ltd, 1 Jan. 2000, <https://jnnp.bmj.com/content/68/1/13>.
6 Mortazavi, Martin M., et al. “The First Posterior Fossa Decompression for Chiari Malformation: the Contributions of Cornelis Joachimus Van Houweninge Graftdijk and a Review of the Infancy of ‘Chiari Decompression.’” SpringerLink, Springer, Dordrecht, 6 Apr. 2011, <https://link.springer.com/article/10.1007%2Fs00381-011-1421-1>.
Cerebrospinal fluid (CSF) is the clear, colorless liquid that surrounds the brain and spinal cord and is contained within a lining called the dura. The cerebrospinal fluid protects and cushions the brain and central nervous system. Among other functions, this fluid provides buoyancy to the brain, allowing it to float and weigh less, thus reducing the pressure at the base of the brain. A cerebrospinal fluid (CSF) leak occurs when there is a tear or hole in the dura that then allows this fluid to escape[1]. When leaks occur, the overall volume and pressure within the skull drops, and the cushioning and buoyancy effect is reduced, causing the brain to slump. In many cases, this leads to a condition known as intracranial hypotension and a vast range of symptoms.
The main symptom of a CSF leak is a headache that is worse when upright and improves when lying down horizontally. This is sometimes called a “positional” or “orthostatic” headache. However, not all positional headaches can be attributed to a CSF leak, and not all CSF leak headaches are positional. This is particularly the case in the chronic (vs acute) phase of CSF leaks, where the “positional” or “orthostatic” characteristic of symptoms may become more constant, lessen, or disappear entirely, including headache. Symptoms often worsen as the day goes on. Other leak symptoms can include, but are not limited to: nausea, vomiting, neck pain or stiffness, heaviness of head, pain between the shoulder blades, feeling of pressure within the head, changes in hearing (muffled or underwater sensation), tinnitus (ringing, buzzing, or pulsatile), feeling of liquid in the ears, sense of imbalance, sensitivity to light, sensitivity to sound, pain or numbness in the arms, changes in cognition (“brain fog,” memory loss, or loss of concentration), dizziness or vertigo, scalp sensitivity or tingling sensation within the scalp, visual changes (blurring, double vision, visual field defects), pain behind the eyes or when moving eyes, facial numbness or pain, sinus pressure, temporomandibular joint pain and stiffness, and subdural hematoma[2]. Cranial leak specific symptoms can vary even more and can include: fluid discharge from ears, nose (usually only one side) and to back of throat often reported as salty or metallic tasting, recurring or chronic meningitis, loss of sense of smell, change in hearing or ringing in the ears, and less frequently cognitive changes. Rare signs or complications of CSF leaks can include: quadriplegia, dementia (often mimicking Frontotemporal Lobe Dementia), Parkinsonism, other movement disorders, ataxia (unsteady gait), hypersomnolence, stupor, coma, stroke (hemorrhagic or ischemic), and even death.
CSF leaks are often very hard to locate, if ever. Approximately 50% of leaks cannot be found on imaging. Imaging and other tests used to attempt to find leaks are often read as “normal” even when there is a leak present. Other times, especially (but not always) in the case of chronic leaks, the positional symptoms either lessen or go away altogether, including the headache. Many who are leaking are not even aware that they are leaking. Leaks are often misdiagnosed as well[3]. Some of those common misdiagnoses are Postural Orthostatic Tachycardia Syndrome (POTS), migraines, sinus headaches, Meniere’s Disease, Chronic Fatigue Syndrome, Parkinson’s Disease (sometimes other neurodegenerative diseases), Fibromyalgia, Ehlers-Danlos Syndrome, Tarlov Cyst, Chiari Malformation, Cervical Spine Disease, cervicogenic headache, tension headache, and Sinusitis. To make diagnosis even more complex and elusive, CSF leaks can and do often occur along with any of these disorders and perhaps several simultaneously. A leak can cause an acquired Chiari malformation or coexist and complicate an existing congenital Chiari malformation[4]. Some patients have had unnecessary decompression surgeries when the underlying, sole cause was a leak all along.
Leaks can be caused by:
Medical procedures (also called iatrogenic leaks) for various diagnostic or therapeutic reasons such as lumbar punctures to collect fluid for analysis if meningitis is suspected, lumbar puncture for injection of contrast (myelography), spinal anesthesia, epidural injections, epidural steroid injections, prior skull base or spinal surgery, CSF shunt over-drainage, prior sinonasal surgery, and chiropractic or other spinal manipulations.
Traumatic injuries such as brachial plexus injuries falls, sports injuries, motor vehicle accidents, roller coaster rides, and other whiplash injuries.
Spontaneous leaks that occur with minimal or no clear cause. Sometimes spontaneous leaks may be associated with some sort of spinal pathologies such as calcified disk material or bone spurs. These leaks are usually ventral (or in front of the spinal cord).
There is growing evidence suggesting that a significant number of spontaneous CSF leaks occur as the result of a preexisting weakness in the dura[5]. Heritable Disorders of Connective Tissues (HDCT’s) such as Marfan Syndrome, Ehlers-Danlos Syndrome (both classical and hypermobility type), autosomal dominant Polycystic Kidney Disease, and other HDCT’s predispose patients to CSF leaks. One leak expert estimates that “slightly less than 100% of patients with spontaneous CSF leaks have an underlying connective tissue disorder.”[6] The dura is made out of connective tissue and patients with HDCT’s have thinner dura mater, that is more susceptible to tears and leaks. HDTC patients are more prone to spinal conditions such as perineural cysts, meningeal diverticula, and other HDCT defects such as aneurysms and dilatations. Oftentimes, a CSF leak is the first sign of an underlying HDCT.
Lumbar punctures (LP’s or spinal taps) should be avoided in patients with Chiari Malformation and/or in patients with HDCT’s[7]. There is a risk of causing a herniation of the cerebellar tonsils or making an existing herniation worse from the pull-down mechanism involved in lumbar punctures. Unfortunately, lumbar punctures are not always avoidable and sometimes very necessary, especially in cases to rule out life-threatening viral or bacterial conditions such as meningitis, subarachnoid hemorrhage, encephalitis, or syphilis. In these cases, measures can be taken to minimize LP risks such as using a certain needle type and size, limit the number of cc’s collected (by spontaneous drip ONLY), and, of course, always done under fluoroscopy by a competent physician[8]. Additionally, it is important to be aware that patients with HDCT’s are at greater risk for the dura to fail to heal following an LP. Patient’s should be aware of post-dural puncture headache (PDPH) symptoms and speak with their physicians if they suspect a leak following an LP.
The procedures and tests used to diagnose leaks will vary between patients and certain criteria are used to diagnose leaks[9]. Some of these tests and procedures might be: endoscopic exam and fluid collection and Beta-2-Trasnferrin testing (cranial leaks), Cisternography (including radioisotope cisternogram), Magnetic Resonance Imaging (MRI) including Magnetic Resonance (MR) myelography, Dynamic CT myelography, Digital Subtraction myelography, and Intrathecal saline infusion-enhanced myelography, a lumbar puncture to collect and test fluid and measure opening pressure. This imaging often includes both brain and spinal imaging. The normal opening pressure is not uncommon and does not rule out a leak. High pressure can also occur while leaking. Pre-existing intracranial hypertension can be related to the development of spontaneous spinal CSF leaks. Some reports suggest that spontaneous cerebrospinal fluid (CSF) leaks are strongly associated with idiopathic intracranial hypertension (IIH). There are 5 main findings on imaging that doctors look for, however, the absence of these findings does not rule out a CSF leak. The mnemonic SEEPS is used for most of these findings: subdural fluid collection, enhancement of pachymeninges, engorgement of venous structures, pituitary hyperemia, and sagging of the brain[10]. Other imaging findings that might be seen are small ventricles, cisterns might have less fluid, optic chasm might flatten over pituitary, pituitary might enlarge, empty sella, fluid in front of the pons, or pons might become flatter than normal. Repeat imaging is often necessary.
Treatment of leaks can either be medical or surgical. Conservative treatment is often recommended, if possible. This can include bed rest and avoidance of coughing, sneezing, straining, bending, twisting, and lifting, increased fluid intake and caffeine, the use of an abdominal binder, and sometimes steroids are recommended. Others may have a lumbar drain placed in the low back to decrease the pressure of the CSF around the area of the leak in an attempt to allow this area to heal. Some patients may need an epidural blood patch. Where a blood patch is not successful, a fibrin glue patch may be tried. About 30-40% of leaks occur at multiple sites, especially in those with an HDCT. Multisite patches may be required. Higher volumes of blood may be needed in order to reach where it needs to go, and/or the position of the needle may need to vary from the standard placement (transparietal or lateral placement)[11]. It is not uncommon for several patches to be tried. Many doctors make the mistake that if an EBP fails, there was no leak as well. Sometimes when more conservative and less invasive treatments have failed, neurosurgery may be necessary. Surgical repairs vary and are tailored according to the type and location of the leak. Sometimes in a select set of patients, other procedures have been used including epidural saline infusions through an implanted epidural catheter or lumbar dural reduction surgery. A condition known as rebound intracranial hypertension (RHP) may occur following any of these treatments[12]. Usually, but not always, there is a different pattern to the headache where one feels worse when horizontal and better when upright. Sometimes, acetazolamide (Diamox) or a similar medication is prescribed to help treat RHP.
Leaks are poorly recognized, poorly understood, under-researched, understudied, often misdiagnosed, can complicate existing conditions, are difficult to find, mimic many other disorders (including Chiari Malformation), and can be comprised of a vast array of symptoms. Most doctors are familiar with the symptoms of a leak in the acute phase. Very few doctors are familiar with how long-term, chronic CSF leaks “present” in regard to headaches and other leak symptoms and often miss the more subtle symptoms of chronic leaks. Like Chiari and other related disorders, no two patients with CSF leaks have the same symptoms and often experience misdiagnosis, delayed diagnosis, are disbelieved concerning their symptoms of the severity thereof, and all too often dismissed to suffer excruciating pain, decline, and debility. Educating yourself as much as possible about CSF leaks will help guide and empower you and those around you who may have existing, suspected or potential future complications that may arise due to CSF leaks.
5 Reinstein, Eyal, et al. “Connective Tissue Spectrum Abnormalities Associated with Spontaneous Cerebrospinal Fluid Leaks: a Prospective Study.” European Journal of Human Genetics, Nature Publishing Group, Apr. 2013, <www.ncbi.nlm.nih.gov/pmc/articles/PMC3598315/>.
7 Erbay, Sami H., et al. “Is Lumbar Puncture Contraindicated in Patients with Chiari I Malformation?” American Journal of Neuroradiology, American Journal of Neuroradiology, 1 Apr. 2005, <www.ajnr.org/content/26/4/985>.
9 Schievink, W. l., et al. “Diagnostic Criteria for Spontaneous Spinal CSF Leaks and Intracranial Hypotension.” American Journal of Neuroradiology, American Journal of Neuroradiology, 1 May 2008, <www.ajnr.org/content/29/5/853>.
11 Griauzde, J., et al. “Large-Volume Blood Patch to Multiple Sites in the Epidural Space through a Single-Catheter Access Site for Treatment of Spontaneous Intracranial Hypotension.”American Journal of Neuroradiology, American Journal of Neuroradiology, 30 Apr. 2014, <www.ajnr.org/content/early/2014/04/30/ajnr.A3945>.
12 Kranz, P. G., et al. “Rebound Intracranial Hypertension: A Complication of Epidural Blood Patching for Intracranial Hypotension.” American Journal of Neuroradiology, American Journal of Neuroradiology, 1 June 2014, <www.ajnr.org/content/35/6/1237>.
![The Important Questions to Ask Your Neurosurgeon [Revised]](https://staging.chiaribridges.org/wp-content/uploads/2023/09/MRI-doctor_AS505903501.jpg)

![Brain Under Pressure – A Guide to Understanding Intracranial Hypertension [Updated]](https://staging.chiaribridges.org/wp-content/uploads/2019/12/Woman_Up-with-headache_AS177290930.jpg)


![Overview: Chiari Comorbidities & Etiological/Pathological Cofactors [Revised]](https://staging.chiaribridges.org/wp-content/uploads/2020/12/DominoEffect_AdobeStock_107422335-copy.jpg)



 But to look at the full history of what became known as a Chiari Malformation, we can begin by looking at the research of a German pathologist, named Theodor Langhans. In his research in 1881 (a decade before Hans Chiari conducted his research on what became known as a Chiari Malformation), while looking at syringomyelia (“a cavity created in the spinal cord”), he noted a “change in the cerebellar cavity.” Upon dissection of the cerebellum, he described the cerebellar tonsils as “two symmetrical pyramidal tumors,” pushing the brainstem forward.
But to look at the full history of what became known as a Chiari Malformation, we can begin by looking at the research of a German pathologist, named Theodor Langhans. In his research in 1881 (a decade before Hans Chiari conducted his research on what became known as a Chiari Malformation), while looking at syringomyelia (“a cavity created in the spinal cord”), he noted a “change in the cerebellar cavity.” Upon dissection of the cerebellum, he described the cerebellar tonsils as “two symmetrical pyramidal tumors,” pushing the brainstem forward. Unfortunately it leaves most of us with failed decompressions, fighting with our neurosurgeons that “something is still wrong.” These neurosurgeons look at their post-operative checklist and see that they successfully did everything surgically required in their out-of-date textbooks:
Unfortunately it leaves most of us with failed decompressions, fighting with our neurosurgeons that “something is still wrong.” These neurosurgeons look at their post-operative checklist and see that they successfully did everything surgically required in their out-of-date textbooks:
