A ligamentous defect in which there is excessive movement between the C1 and C2 vertebrae (usually rotational) and can result in neurological symptoms and deficits.
Most Chiarians go to see a surgeon with an expectation of them being knowledgeable in their field. However, while they might be a neurosurgeon, their knowledge of Chiari and its comorbid/pathological conditions might not rank high in their practice. Make the most of your initial appointment by interviewing them and what they really know about Chiari Malformations. Be cautious of inflated success rates. Chiari decompression in general offers a just over a 50% success rate (which means it has a nearly 50% failure rate). Surgeons that claim a 100% (or near 100% success rate) are usually not basing their success on how their patients feel afterward, it is based on if they were successful with the aspects of the surgery: Removal of the occipital bone ✓ Opening the dura and adding the patch/graft ✓ Laminectomy ✓ Cauterization/resection of cerebellar tonsils ✓
WE DESERVE BETTER THAN THAT!
HERE IS A LIST OF CHIARI QUESTIONS WE RECOMMEND ASKING AT YOUR FIRST NEUROSURGERY APPOINTMENT:
General Questions:
How do you define a Chiari Malformation?
What do you believe causes a Chiari malformation?
Are all Chiari malformations from a small posterior fossa?
Do I have a small posterior fossa? If yes, how big is it? If size is unknown, was my posterior fossa measured? If not, why not? How did you come to the conclusion that I have a small posterior fossa?
How common do you believe Acquired Chiari malformations to be?
Do you always recommend decompression surgery for all of your patients with herniated cerebellar tonsils? Why/why not?
In an average month, how many Chiari decompressions do you perform? How many tethered cord releases? How many craniocervical fusions? What percentage of your practice is spent treating patients with these connective tissue related conditions?
Looking at my brain scan, is any part of my “brainstem” herniated (below the posterior fossa)? If so, does that make me a Chiari 1.5?
Intracranial Hypotension (low pressure) Questions: *Article to help you understand CSF Leaks & Intracranial Hypotension prior to your appointment. If you have SYMPTOMS OF LOW INTRACRANIAL PRESSURE and/or suspect a cerebrospinal fluid leak, we recommend asking the following questions:
S.E.E.P.S.
Looking at my brain scan, do you see any Subdural fluid collections?
Looking at my brain scan, do you see an Enhancement of pachymeninges?
Looking at my brain scan, do you see an Engorgement of my venous structures? Should we do an MRV to make sure?
Looking at my brain scan, does my Pituitary appear to be enlarged?
Looking at my brain scan, does my brain appear to be Sagging?
Looking at my corpus callosum:
Does there appear to be a depression?
Is there an inferior pointing of the splenium?
If he/she answers affirmatively to any of the above S.E.E.P.S. questions, ask:
What should be done to find/repair a potential leak?
Are you aware that it is common for CSF Leaks to not show up on MRI?
Are you willing to do a CT Myelogram and/or a digital subtraction myelogram, if I develop symptoms of a leak and none can be found on MRI?
Are you aware that it can often take multiple epidural blood patches to try and seal a leak, and sometimes when a blood patch fails to work, a surgical dural repair might be necessary?
Intracranial Hypertension (high pressure) Questions: *Article to help you understand Intracranial Hypertension prior to your appointment. If you have SYMPTOMS OF HIGH INTRACRANIAL PRESSURE, we recommend asking the following questions:
Looking at my brain scan, do I have cerebrospinal fluid in my sella turcica (Empty Sella Syndrome)?
Looking at my brain scan, do you see any evidence of my optic nerves are swollen (papilledema)?
If so, should I be referred to a neuro-ophthalmologist?
Looking at my brain scan, do my lateral ventricles appear small or flattened?
If so, do I need to have my pressures checked?
If yes, are you aware of the risks of developing a CSF Leak from a lumbar puncture?
What are the symptoms of a CSF Leak, should one develop?
What is your plan of action if I should develop these leak symptoms?
Are you aware that it is common for CSF Leaks to not show up on MRI?
Are you willing to do a CT Myelogram if I develop symptoms of a leak, and none can be found on MRI?
Should a leak be found, are you aware that it can often take multiple epidural blood patches to try and seal a leak?
Tethered Cord Questions: *Article to help you understand Tethered Cord: Sorry, Coming Soon. If you have SYMPTOMS OF TETHERED CORD, we recommend asking the following questions:
Looking at my brain/cervical scan, does my brainstem appear to be elongated?
Looking at my cervical scan, does my spinal cord appear to be stretched?
Looking at my lumbar scan, does my conus reach my mid/low L2?
Looking at my thoracic and lumbar scan, does my spinal cord appear to be pulling to the back, or one particular side?
If so, should we do a prone MRI to see if it has actually adhered to that side?
Looking at my lumbar scan, do I appear to have fatty tissue inside the epidermis?
If the answer to any of these questions is affirmative, do you suspect that I have a tethered spinal cord?
If so, should we plan for a Tethered Cord Release before or soon after decompression surgery, so the likelihood of a failed decompression is reduced?
If I have urological issues, can I get a referral for urodynamic testing to rule out any other potential causes of my urological issues?
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI): *Article to help you understand CCI & AAI prior to your appointment. If you have SYMPTOMS OF CRANIOCERVICAL INSTABILITY or SYMPTOMS OF ATLANTOAXIAL INSTABILITY, we recommend asking the following questions:
Looking at my brain/cervical scans, what are the measurements of my clivoaxial angle and Grabb-Oakes?
Do these measurements meet the diagnostic criteria for Craniocervical Instability?
Looking at my flexion and extension imaging, how many millimeters of translation are there between flexion and extension?
Does Chamberlain’s Line cross my odontoid? If so, does it cross at a level that would indicate Basilar Invagination?
Looking at my rotational imaging, what is the percentage of uncovering of the right and left articular facets on rotation?
Do the percentages from my rotational imaging meet the diagnosis criteria for Atlantoaxial Instability?
IF A DIAGNOSIS CRITERIA IS MET IN ANY OF THE ABOVE, WE STRONGLY RECOMMEND THAT YOU WAIT ON DECOMPRESSION AND PURSUE THE TREATMENT OF SAID CONDITION(S) AND THAT OF EHLERS-DANLOS SYNDROME, AS EACH OF THESE CONDITIONS CAN BE PATHOLOGICAL TO AN ACQUIRED CHIARI AND EACH IS A STRONG INDICATOR THAT A CONNECTIVE TISSUE PROBLEM EXISTS.
*The questions in this article will periodically change as we are able to expand our recommended questions.
*Original version released September 2018, revised 2023.
When you start to educate yourself on a condition like Chiari, your vocabulary will be challenged. Most of us study with a medical journal article opened in one tab and medical dictionary in the next. Amongst all the medical terminology you will tackle, there are probably a few terms as important to your understanding of Chiari than comorbidities and pathological/etiological cofactors. When two or more conditions tend to co-occur, they are said to be comorbid with one another. It makes no inferences of a causal relationship between the conditions, only that they co-occur. This co-occurrence deduces that a correlation exists, but when the nature of that correlation is not known, they are just said to be comorbidities. When a “causal relationship” is known or suspected, the conditions start being discussed in terms of pathology or etiology, which are similar, but not exactly the same thing.
An etiological cofactor exists when the “root cause” of a condition is known or believed to be known. That “root cause” is the etiological cofactor. When an etiological cofactor can cause a series of events or conditions that can become “direct causes” for other conditions, that series of events creates a pathology. Conditions along the path are called pathological cofactors. Understanding these cofactors is imperative in understanding Chiari and all of the comorbid conditions that accompany it.
ETIOLOGICAL COFACTOR:
Chiari Malformation often seems like a beast that wreaks havoc on our bodies on every level. Indeed it is, but as you can see from the diagram above, it really is not the “root” of everything that is going wrong. There is a bigger beast at work in so many of us, and its name is Ehlers-Danlos. It is not by chance that so many of us with Chiari have so many other conditions in common (especially conditions like Degenerative Disc Disease, arthritis and other connective tissue problems). It is not by chance that so many of us have a history of miscarriage and similar familial histories. It is not by chance that Chiari is more prevalent in females than males. And it is definitely not by chance that Chiari is running in families and they cannot find a definitive genetic link. They cannot find it because they are not looking at the beast hiding in the background.
Ehlers-Danlos Syndromes are a group of inherited disorders involving a genetic mutation in one or more of our bodies’ collagen. Collagen is the most abundant protein, making up 1/3 of the proteins in the human body, affecting our bones, skin, muscles, and connective tissue[1]. Collagen is often described as a “cellular glue” that helps hold the body together. When that glue fails to hold, everything seems to go awry; before and after birth: skulls can under-develop in utero, organs tend to prolapse, and bones begin to shift as joint laxity increases (including the bones/vertebrae at the craniocervical junction). Ehlers-Danlos is a primary “root cause” of Chiari Malformations and a majority of the other problems we have. The list in blue is far from being a complete list of conditions caused by EDS. They are commonly accompanied with Chiari because they can cause or attribute to a Chiari malformation (pathological cofactors).[2]
PATHOLOGICAL COFACTORS:
Cranial Settling occurs when the skull has dropped and the odontoid (C2/axis) enters into the foramen magnum (Basilar Invagination). This drop can further compromise the craniocervical junction and as it pushes everything down, it increases the likelihood of an Acquired Chiari Malformation.
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI) usually occurs with cranial settling and Basilar Invagination (BI). The settling and/or softening of tissue can cause a shifting of the C2 (resulting in CCI or AAI) and the cerebellar tonsils (which are already inclined to prolapse) simply drop down with each shift affecting ones ability to tilt/rotate their head.[3]
Intracranial Hypertension (IH – High Intracranial Pressure) occurs when your intracranial pressure (ICP) becomes elevated. This elevation can happen for a variety of reasons.
Space Occupying Masses (cysts, tumors or hydrocephalus) take up space inside the skull causing a “mass effect.”
When no mass effect exists, many doctors look no further and give the diagnosis of Idiopathic Intracranial Hypertension.
Because the area of the skull is fixed in an adult cranium and partially fixed in that of a child, the elements inside the fixed space (CSF, blood volume and brain matter) tend to get pushed out wherever they can (the only place that they can escape without breaking through the dura is through the foramen magnum and the brain matter that’s closest to the foramen magnum is the cerebellar tonsils).[4]
Tethered Cord Syndrome occurs when the tissue inside the epidermis adheres to the spinal cord or filum terminale. While this tethering can happen anywhere along the spinal canal, it is most common in the lower lumbar and/or sacral spine. When this adhesion happens it creates a pulling down of the spinal cord and consequently, the brainstem located at the top of the spinal cord and the cerebellar tonsils just get pulled down with it.[5]
Intracranial Hypotension (Low Intracranial Pressure, often involving a CSF Leak) usually involves a cerebrospinal fluid leak or an over-draining shunt, we will highlight the former. Ehlers-Danlos patients tend to have weak dura matter. Tears/holes in the dura can happen anywhere in the dura surrounding the brain or spinal canal and they can happen completely spontaneously (without a known cause). When the leak occurs in the spinal canal, they can create a suctioning effect where cerebrospinal fluid (CSF) is being pulled down and out, causing the intracranial pressure (ICP) to drop. The cerebellar tonsils that are already prone to prolapse (due to EDS) end up getting suctioned downward with the CSF.[6] Cranial leaks often happen when high pressure is left untreated until the high pressure causes a leak in the dura mater. In cranial leaks, fluid usually leaks through the nose or ears (less common), and you can often taste the metallic taste of the cerebrospinal fluid in the back of your throat. While both spinal leaks and cranial leaks can cause low pressure and low-pressure symptoms, and while both can start, stop, and start again spontaneously, there is an increased risk whenever there is an opening where cerebrospinal fluid leaks outside of the human body (if cerebrospinal fluid can make it out of the body, microscopic bacteria can make it inside the same opening where it can enter in the meninges).[7]
Posterior Cranial Fossa Hypoplasia (PCFH) is the only etiological cofactor listed above that is definitely congenital. The role of collagen in bone development has been long-standing, especially its known contribution to certain conditions like Osteogenesis Imperfecta. However, more recent studies are discovering the role collagen plays in congenital posterior fossa anomalies. Posterior Cranial Fossa Hypoplasia is the most commonly “acclaimed” cause of Chiari malformations, but studies show, that even when all of the other causes above are factored out, only approximately 52% of those left (that fail to meet “the diagnosis criteria” for any of the above), have a small posterior fossa.[8]
COMORBIDITIES:
While all of the conditions listed in the diagram are comorbidities, some are etiological/pathological of an Acquired Chiari (even though nearly 100% of us are told that our Chiari Malformation is congenital) and others have Chiari Malformation as their etiological/pathological cofactor:
Syringomyelia occurs when cerebrospinal fluid (CSF) is obstructed and a CSF filled cyst/cavity forms inside the spinal cord. This cyst is directly related to the obstruction of cerebrospinal fluid that can be caused by Chiari Malformation, Spinal Stenosis (a narrowing of the spinal canal, spinal cyst/tumor, a herniated disc), or irregular curvature of the spine (scoliosis). When that cyst/cavity extends into the medulla oblongata (the lowest part of the brainstem), it is called Syringobulbia, and it comes with a new set of symptoms consistent with the damage being done to the brainstem. So when Chiari Malformation exists with a syrinx, and there is no stenosis or disc problem in close proximity below it, the Chiari Malformation should be listed as the etiological condition of the syrinx. If more than just the Chiari Malformation is believed to be causing the syrinx, each would be more accurately described as pathological.
Dysautonomia occurs when damage has been done to the brainstem or Vagus nerve. Whenever either of these is damaged, often from compression at/near the craniocervical junction, the autonomic nervous system can begin to dysfunction.
Confused? If you understand the causal relationships but find yourself wondering if a comorbid condition is an etiological or a pathological, think of it in terms of a domino effect. Only the first domino is etiological. All of the dominoes in between (on the path) are pathological. The important thing to remember in this array of medical terminology is that while everything is definitely not Chiari, it almost always shares a connection to it, and that is why so many of us have so many conditions and symptoms that doctors call unrelated! It is imperative in our fight that we know “what” we have and “why” it is happening. With such a broad spectrum of symptoms (like we all have), we must educate ourselves and not just believe the limited knowledge of our doctors.
7 Pérez, Mario A et al. “Primary Spontaneous Cerebrospinal Fluid Leaks and Idiopathic Intracranial Hypertension” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4 (2013): 330-7. doi:10.1097/WNO.0b013e318299c292, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>
Today is 11th April, 2019. Spring is in the air, yet I struggle to appreciate its presence. My daughters are at school, my son is at home in bed yet again. Like so many other days he is unable to get up. My son is 19 years old and looks just like any other 19 year old. You would never guess that this 19 year old is fighting a tremendously unfair battle every single day and has done so for several years.
Let me rewind.
My son was around 9 years old when he first complained of a lack of feeling on his right side and regular headaches. Doctors in Ireland, where we were living at the time, told him to drink more fluids after his daily soccer practice and put the numbness down to a trapped nerve. When he was 14 years old and living in Canada, he was told exactly the same by doctors there. However, when I finally insisted on him being referred to a neurologist, this very neurologist laughed at my son for wasting his time. He was told that it was all in his head. I vividly remember telling him off myself in the carpark on our way home.
I also remember being disappointed about his worsening school reports, blaming the onset of teenage years for his inability to concentrate and retain information. Blurred vision was also dismissed when his eye test came back just fine. Doctors didn’t grow concerned until he was 16 years old and living in France when a routine soccer medical check-up showed a sudden scoliosis deterioration from 8 degrees to 40 degrees. Subsequent MRIs showed Chiari Malformation (CM) with extensive Syringomyelia.
Neurosurgeons were quick to reassure him that all should be fine after a decompression surgery. Nevertheless, I spent hours researching these unknown rare conditions and found two experienced neurosurgeons, one in England and one in Belgium, for second opinions. Whereas surgeons in France took a more traditional approach and talked about inserting a shunt, both these surgeons warned strongly against this and so we made the decision to go to Belgium for the surgery. We felt well informed and were full of hope when my son embarked on his healing process 3 years ago.
Let me tell you where we are now.
Doctors in Europe tell us that my son is one of the unlucky few as his health has drastically deteriorated. Scar tissue has attached itself to his brain tonsils but that only explains part of his deteriorated health. So I embarked on a mission to get to the bottom of these problems. Surely there was hope to be found in the health system in France, one of the best in the world! After countless appointments with multiple health professionals, we were dumbfounded by the complete lack of understanding, knowledge and pure arrogance in relation to CM and its associated conditions, which resulted in my son’s mental health being questioned yet again.
I started carrying out my own research, which clarified the distinct link between brain disorders and compromised immune/digestive systems. Whereas his doctors are reluctant to make that link, the evidence is clear. 18 months after surgery, my son got struck down by glandular fever. Again, we were hopeful that this would only be a temporary setback. Today however, my son suffers from chronic fatigue syndrome as well as dysautonomia.
At our wits end last summer, we turned to a hospital in the United States that specialized in Chiari Malformation. Our first consultation with its Managing Director turned out to be an eye opener. This neurosurgeon could literally finish our sentences. My son was finally understood. It turns out that doctors in Europe had failed to diagnose another condition, Ehlers-Danlos Syndrome (EDS), which caused craniocervical instability. This in itself can be a debilitating condition but the combination of craniocervical instability with brain decompression surgery can be a death sentence. He further explained that such patients are deemed to benefit from Occipitocervical Fixation (OC) Fusion surgery. However, this surgery has not yet received the green light for these conditions from Health Services in Europe.
Armed with a diagnosis of Complex Chiari, we faithfully returned to my son’s French doctors, only to be met, yet again, by a lack of understanding. My request for an upright flexion/extension MRI was seen as outlandish and peculiar. Turns out, an upright MRI is not yet available in France. Instead they still rely on flexion/extension X-ray images which fail to adequately detect craniocervical instability.
In recent discussions, our son’s Belgian neurosurgeon cautiously recognizes the link between CM and EDS. However, as these studies are in their infancy in Europe, doctors still carry out decompression surgeries without checking for EDS. He also questions the durability of an OC Fusion but agrees that much more extensive research needs to be carried out in Europe and that my son is extremely unfortunate this hasn’t happened yet.
So where does this leave my son? In the land of limbo. Knowing that Europe is trailing some 10 years behind the States in this field. France, with its inherent reluctance to change, probably closer to 15 years. School is no longer an option for my son as his brain fog and memory loss have become more and more of a problem, his fatigue too debilitating and his headaches too frequent.
We are tired of fighting the system, tired from having to spell out the name of his conditions to health professionals, tired of being misunderstood. There are days I avoid going out as I don’t want to answer people’s well-meant questions. There are days I am ashamed of the anger that wells up inside me when friends air their worries about their children’s school results. There are days I feel like I am being punched in the stomach when I see his friends play a soccer match. People tell me I am strong. I don’t agree. I wish I had been strong all those years ago and believed my son over his doctors.
My son is my hero. My son is a fighter. My son has generally done what health professionals told him to do, taken every medication health professionals told him to take, followed the advice health professionals told him to take, yet the system continues to let him down. When I look into my son’s eyes, I still see this steadfast determination but I now also see pain and disillusionment. My son believed me when I told him we would overcome this together. My son believed me when I told him the worst would be over soon. My son doesn’t believe me anymore. I feel that I have failed him.
Complex Chiari diagnosed so late is a life sentence. It has brought pain, sadness and isolation, not only to my son but to my entire family. My husband and I are learning to compartmentalize, enjoy moments. We live in hope that our son’s better periods will begin to lengthen and pick ourselves up every time these come to an abrupt end. We have to. We owe it, not only to our son but to our daughters too.
We continue our journey through the unknown, thankful for the sources of information coming from the United States, usually met with skepticism and resistance by French health professionals. However, one thing I have learned from our journey so far is that we cannot fight these conditions and health services alone. Surely there must be more people out there in Europe. Surely, as a group we can start making a difference. Let’s unite! Let’s educate! Let’s raise awareness! Our children deserve so much better! Our children deserve to be heard, supported, and at the very least, understood!
THE DEFINITION OF A CHIARI MALFORMATION HAS BEEN LONG DEBATED. IT REALLY IS NO WONDER THAT PATIENTS AND MEDICAL PROFESSIONALS ALIKE ARE CONFUSED. THEN, WITH US FULLY UNDERSTANDING ALL SIDES OF THE DEBATE, WE DEFINED A CHIARI MALFORMATION AS STRUCTURAL DEFECTS IN WHICH THE CEREBELLUM, THE HIND PART OF THE BRAIN, DESCENDS BELOW THE FORAMEN MAGNUM INTO THE SPINAL CANAL. THIS DEBATE IS BEING ANALYZED THIS YEAR, AS CERTAIN ORGANIZATIONS ARE BRAVING TO ATTEMPT TO BRING DOCTORS ALL UNDER ONE UNIFORM DEFINITION AND DIAGNOSTIC CRITERIA. THEREFORE, AMIDST ALL THE CONFUSION AND DEBATE, WE WANTED TO EXPLAIN THE FACTORS INVOLVED, AND WHY WE WENT WITH THE DEFINITION THAT WE DID, AND WHY ONE STANDARD IS SO IMPORTANT!
To better facilitate our explanation, we will call all associated terms by their specific medical names:
Tonsillar Ectopia (TE) = tonsillar herniation of any size Posterior Fossa Hypoplasia (PFH) = an underdeveloped posterior fossa
Chiari Malformation Vs. Arnold Chiari Malformation
The most common type of Chiari is Type 1 (which includes a Chiari 1.5, where the brainstem is also below the foramen magnum). Many people use the term “Chiari Malformation” when diagnosed with Type 1, while others cling to the name “Arnold Chiari Malformation” with the same diagnosis. Is there a difference? The name “Chiari Malformation” came from Hans Chiari, an Austrian pathologist, who first discovered the malformation in the late 19th century.[1, 2] Julius Arnold, a German pathologist, later expanded on Chiari Type 2, and Type 2 took on his name “Arnold Chiari Malformation.” Therefore, technically speaking, a Chiari Malformation and an Arnold Chiari Malformation are not the same; Arnold Chiari Malformation is specific to Chiari Type 2 (which usually includes a myelomeningocele, the most serious form of Spina Bifida). However, they are used interchangeably by many, even by medical professionals and the misnomer is of little consequence one way or the other.[3]
Chiari Malformation = Posterior Fossa Hypoplasia Theory
Many ascribe to the theory that a Chiari Malformation ONLY consists of a posterior fossa hypoplasia (which means that the back of the skull is malformed, and therefore the cranial area (space) at the rear is too small). They believe that a tonsillar ectopia is only a symptom, and a Chiari Malformation can exist with or without an accompanying ectopia. This argument is not without merit, because much of what was initially being looked at by Hans Chiari were deformities in the posterior skull upon postmortem examination (so there wasn’t soft tissue to analyze). He originally attributed much to hydrocephalus, but expanded his research into the pons, medulla oblongata, and cerebellum (which can all be attributed to intracranial pressure as a pathology of a “tonsillar ectopia”). To ascribe to this belief would also mean that “Acquired Chiari Malformations” cannot exist, as one doesn’t “acquire” a small posterior fossa. And that would also mean that Chiari Type 2, Type 3 and Type 4 technically would not be a Chiari Malformation at all either, since their definitions do not require a posterior fossa hypoplasia. Perhaps type 3, which has an opening at the back of the skull, but no “small posterior fossa” is even implied in the definitions.
But to look at the full history of what became known as a Chiari Malformation, we can begin by looking at the research of a German pathologist, named Theodor Langhans. In his research in 1881 (a decade before Hans Chiari conducted his research on what became known as a Chiari Malformation), while looking at syringomyelia (“a cavity created in the spinal cord”), he noted a “change in the cerebellar cavity.” Upon dissection of the cerebellum, he described the cerebellar tonsils as “two symmetrical pyramidal tumors,” pushing the brainstem forward.[4] In fact, the other noted researchers: Nicholas Tulp (1593–1674), John Cleland (1835–1925), and Julius Arnold (1835–1915), all centered on the hindbrain hernia [herniation] without speculation as to its etiology/pathology. It is said that “many of the English translations of Chiari’s work contain inaccuracies.” But note that Chiari’s first paper was on “ectopia of cerebellar tissue,” and that he went on to define Type 1 as showing, “elongation of the tonsils and medial parts of the inferior lobes of the cerebellum into cone shaped projections, which accompany the medulla oblongata into the spinal canal.”[5] Which sounds like what is now known to be a Chiari 1.5. Much later, in 1938, at a time when the posterior fossa decompression became the popular surgical treatment for a Chiari Malformation, a Chiari 2 patient “underwent posterior fossa exploration with the authors not considering hindbrain herniation in their differential. Penfield and Coburn later stated that: ‘In retrospect it seems that we should have suspected the Arnold-Chiari malformation. Instead, a suboccipital craniotomy was carried out…” So even the early neurosurgeons seeking to perfect their surgical treatment felt that it was a mistake to concentrate on the posterior fossa and not take into account etiologies of the hindbrain herniation. That mistake is still going on 80 years later.[6]
The biggest problem that they are going to have with strictly defining a Chiari Malformation as a small posterior fossa resides in the fact that the diagnosis criteria for a Chiari Malformation only consists of ONE MEASUREMENT, the length of the tonsillar ectopia (how far the tonsils herniate below the foramen magnum). Generally, there are no measurements of the posterior fossa taken when radiologists make the initial diagnoses. Furthermore, most neurosurgeons see the radiology reports, and depending on symptomology, they make the decision to decompress or not to decompress without ever measuring the size of the posterior fossa. Most never look for (and often do not know about) etiological/pathological cofactors that could have been causing the tonsillar prolapse in the first place.
Where does this assumption leave us?
Unfortunately it leaves most of us with failed decompressions, fighting with our neurosurgeons that “something is still wrong.” These neurosurgeons look at their post-operative checklist and see that they successfully did everything surgically required in their out-of-date textbooks:
Suboccipital bone was appropriately decompressed. ✔️
Dura was opened and dura patch was successfully inserted. ✔️
Lamina was successfully removed from the C1 (and sometimes the C2 as well). ✔️
They did all that was required of them based on the diagnoses presented! They don’t have time (or don’t care) to look beyond that, so once again, the idea of our continued symptoms are thought of as being psychosomatic.
While we applaud the efforts of those seeking to get a measure of consistency in how Chiari is defined, the truth remains that until the diagnosis criteria is changed as well, we are being diagnosed with Chiari Malformation based on our tonsillar herniation; it is presumed to be congenital; we are being surgically treated as though it is congenital, and we are ending up with failed decompressions. This confusion is beyond unacceptable, it’s reprehensible!
When it is all redefined, hopefully we will have a well defined diagnosis criteria, or it is all irrelevant. And the many that really did acquire what was assumed to be “congenital” who are now being told that they do not have Chiari Malformation at all, will be able to get lawyers for “an improper diagnosis” that lead to the incorrect brain surgery being done. There are surgeons coming around and finally seeing that there is merit to these studies that have been done since the late 1990s, that have shown a pushing/pulling effect that can cause the tonsillar ectopia that gets us diagnosed with a Chiari Malformation, and we applaud them for having the integrity to stand up and get it right. That’s exactly what we need and deserve!
If you were diagnosed with a Chiari Malformation and want to know how all of this might be affecting you, we encourage you first to find your initial radiology reports, and see if there were measurements taken of the posterior fossa. And then wait with that information… wait and see what changes are actually made to the definition. While you are waiting learn. Learn everything you can about every etiological/pathological cofactor, and every comorbidity. If it is “officially” redefined as a small posterior fossa, we will have to work together as a community (like we always do) to help lawyers see how we have been getting lost in the shuffle, year after year. If it’s not officially changed and Chiari continues to be defined as a structural defect involving the cerebellar tonsils, we will have to continue in our fight to make these cofactors of Acquired Chiari Malformation known!
4 Mortazavi, M M, et al. “The First Description of Chiari I Malformation with Intuitive Correlation between Tonsillar Ectopia and Syringomyelia.” Advances in Pediatrics., U.S. National Library of Medicine, Mar. 2011, <https://www.ncbi.nlm.nih.gov/pubmed/21361763>.
5 Pearce, J M S. “Arnold Chiari, or ‘Cruveilhier Cleland Chiari’ Malformation.” Journal of Neurology, Neurosurgery & Psychiatry, BMJ Publishing Group Ltd, 1 Jan. 2000, <https://jnnp.bmj.com/content/68/1/13>.
6 Mortazavi, Martin M., et al. “The First Posterior Fossa Decompression for Chiari Malformation: the Contributions of Cornelis Joachimus Van Houweninge Graftdijk and a Review of the Infancy of ‘Chiari Decompression.’” SpringerLink, Springer, Dordrecht, 6 Apr. 2011, <https://link.springer.com/article/10.1007%2Fs00381-011-1421-1>.
Craniocervical Instability and related pathologies of the craniocervical junction are an important topic for anyone diagnosed with Chiari 1 malformation. “Complex Chiari,” or the presence of craniovertebral abnormalities or instability in addition to the presence of cerebellar tonsillar herniation, is present in approximately one fourth of all cases of Chiari 1 malformation[1]. These cases usually involve the presence of a genetic connective tissue disorder and are thought by experts to be the cause of most Chiari decompression failures[2]. When the doctor and patient alike are not knowledgeable about these conditions and the additional symptoms that often accompany them, these more complex cases are often treated with a standard decompression, which can actually weaken the stability of the craniocervical junction more, and result in an increase of symptoms rather than a clinical improvement. Understanding what signs and symptoms to look for that may indicate that your Chiari is more complex, is vital in receiving the appropriate treatment the first time. This is especially important considering that, according to Chiari expert Paolo Bolognese, M.D., “[with revision surgeries], the results are not as good as if you had done the posterior decompression well the first time.”[3]
Punjabi and White define instability as the “loss of the ability of the spine under physiological loads to maintain relationships between vertebrae in such a way that there is no damage or subsequent irritation of the spinal cord, (brain stem) or nerve roots, and in addition that there is development of deformity or incapacitating pain due to structural changes.”[4] This means that the ligaments and muscles that normally hold the spine together, are too weak or damaged to handle the normal range of motion and weight of anatomic structures. For example, in Craniocervical Instability, the neck is not strong enough to support the normal weight of the head, without elements of the spine moving in such a way that it causes pain or damage to the nervous system (spinal cord, brain stem, and even cranial nerves). The result is that the bones that make up the lower skull and upper spine get pushed out of their normal anatomic location and begin to impinge on or cause stretching of these parts of the nervous system.
Craniocervical Instability can result from or be exacerbated by a trauma, such as a severe whiplash injury. However, many cases of CCI are associated with some sort of connective tissue disorder, such as a heritable disorder of connective tissue (HDCT, like Ehlers-Danlos Syndrome or Marfan’s), or an autoimmune condition that affects the connective tissue (such as Rheumatoid Arthritis), or a few other rarer conditions that affect the integrity of bony structures in the skull and spine. Instability can result either from lax ligaments and other connective tissues, soft bones (also seen in HDCTs) or from something like pannus formation, where repeated rubbing together of the joints causes a build-up of granulated tissue around bony structures and changes the way certain bones lie in relationship to one another[5]. Craniocervical Instability can also result as a complication of Chiari decompression surgery, when too much bone is removed from the skull, resulting in the instability of the skull on the top of the spine[6].
In the patient community, the term “CCI” is often used in reference to both Craniocervical Instability and Atlantoaxial Instability (AAI). CCI is often used to refer to the commonly seen combination of issues with the craniocervical junction, that include the instability of the joints where the skull meets the C1 vertebrae (which is true CCI), the instability of the joints between C1 and C2 (true AAI), a retroflexed odontoid, pannus formation, and a kyphotic clivo-axial angle (which are all forms of basilar impression/invagination). But CCI really should refer to the movement of the skull with respect to the spine. This sliding is referred to as “translation” and is measured on dynamic imaging in millimeters. The pathological threshold for the degree of translation of the basion with respect to the odontoid process between flexion and extension is 2mm, and any amount of translation greater than 1mm is capable of producing symptoms7. Likewise, at the C1-C2 joint, instability in the form of AAI can cause an excessive uncovering of the joint facets. Facets are the surfaces of the vertebrae that articulate with next vertebra. An uncovering of the facets that exceeds 20% is considered pathological.
The occipito-atlantic joint allows for about half of the cervical spine’s ability to flex and extend (tilt forward and backward). Likewise, the atlantoaxial joint [the articulation between C1 (atlas) and C2 (axis)] accounts for about half of the cervical spine’s ability to rotate the head. Because of this, these vertebrae lack the same amount of stability as the remainder of the spine, and ligaments are largely responsible for their stability[8]. Therefore, ligamentous laxity, as seen in connective tissue disorders, make these areas of the spine particularly prone to pathologic instability. Symptoms of AAI may include visual changes, syncope (fainting) or near-syncopal episodes, dizziness, nausea, facial pain, difficulty swallowing, choking, respiratory issues, and upper cervical tenderness. These symptoms will usually improve with the use of a neck brace[9]. For patients with connective tissue disorders, as are seen in 12-20% of patients diagnosed with Chiari, dynamic imaging is very important in identifying potential instability. The ideal tests to diagnose CCI and AAI are an upright MRI with flexion and extension and a 3D CT with rotational views, respectively[10]. It is important to note that ventral brain stem compression may not be seen on traditional supine MR imaging, while it may be very evident on dynamic imaging.
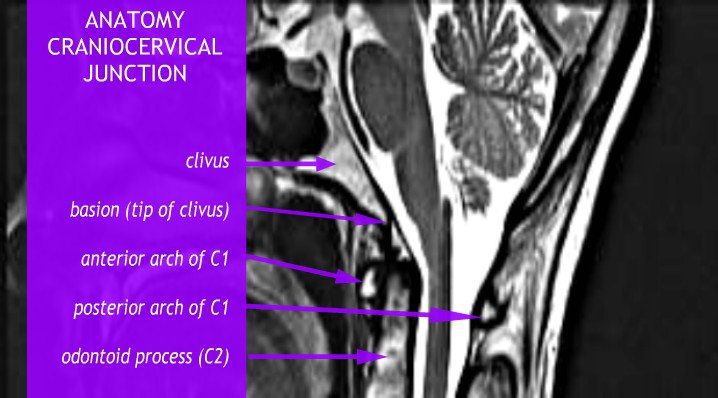
Basilar Invagination and Basilar Impression are also often seen with instability. They are almost identical to one another, and refer to upward displacement of the bones of the spine. However, technically, Basilar Invagination is caused by this deformation with normal bone, while Basilar Impression results from softening of bone[11]. For our purposes, this distinction is less important, but we will discuss any displacement in terms of “Basilar Invagination,” or “BI” for short. Forms of Basilar Invagination now include the prolapse of the odontoid process through the foramen magnum (the original condition described by the term), cranial settling, a kyphotic clivo-axial angle, and a retroflexed odontoid[12]. The kyphotic clivo-axial angle is an important and relatively easy measurement to indicate potential deformative stress on the brain stem. The clivus is a wedge-shaped bone that normally lies above and ventral to the top of spine. When it lies more horizontally, it creates a sharp angle that results in a bending of the brainstem. The odontoid peg (also called the odontoid process or the dens) is the part of the C2 vertebrae, or Axis, that the skull pivots upon, so named because of its tooth-like shape. A retroflexed odontoid occurs when the odontoid is bent backwards, often compressing the front of the brain stem. Other important measurements involving ventral brain stem compression for a kyphotic clivo-axial angle and/or retroflexed odontoid include the Grabb-Oakes and Harris measurements.
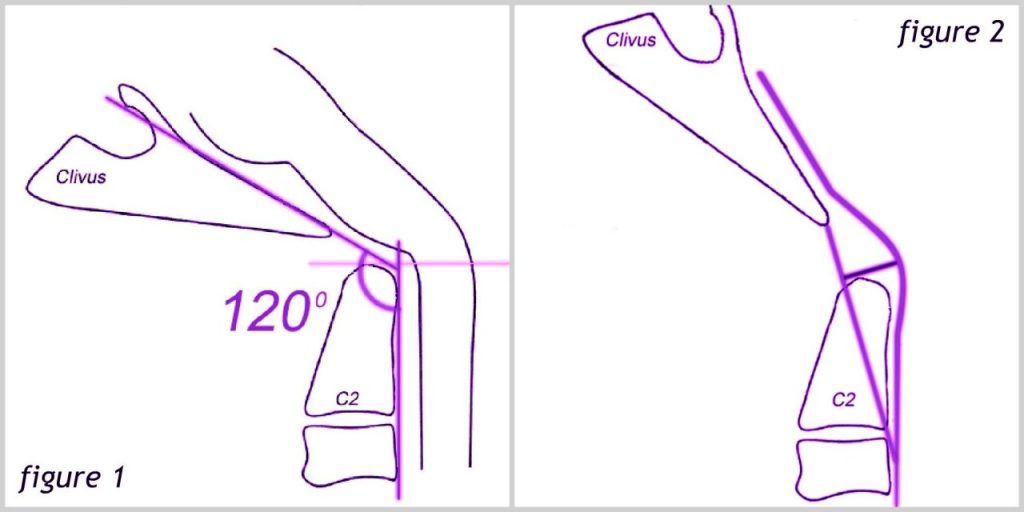
The clivoaxial angle is measured by drawing a line along the posterior (back, or when lying more horizontal, the top) side of the lower clivus and intersecting that line with a line drawn on the posterior side of the axis. If the angle created is less than 135°, it is considered pathological. Like instability, a kyphotic clivoaxial angle is often seen in patients with connective tissue disorders and degenerative rheumatoid disease[13]. See figure 1 below.
Left – Clivoaxial Angle (CXA). Right – Grabb-Oakes measurement.
For the Grabb-Oakes measurement, a line is drawn from the basion (the midpoint of the anterior margin of the foramen magnum) to the inferior posterior C2. A perpendicular line is then drawn from the center of this line to the dura of the brain stem. A Grabb-Oakes measurement greater than 9 mm denotes a form of basilar invagination. This is a very helpful measurement for determining how much a retroflexed odontoid is compressing the brain stem. See Figure 2 above.
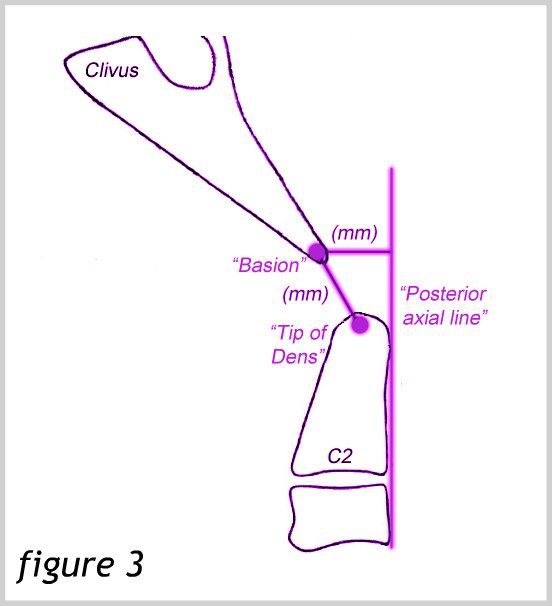
The Harris measurement is the distance between the basion and the Posterior Axial Line. This distance should not be more than 12 mm. A measurement of more than 12 mm also denotes instability. This measurement can also be used to measure the translation between flexion and extension in dynamic imaging[14]. See Figure 3.
Harris measurement
Symptoms of ventral brain stem compression can occur with various types of BI and instability. They may be referred to together as a “cervicomedullary syndrome” and may include[15]:
A heavy headache (often referred to as feeling like a “bobblehead” or feeling like the head is a “bowling ball”)
A Chiari-type pressure headache aggravated by Valsalva maneuvers (because these conditions, like Chiari, can also cause flow issues)
Facial pain or numbness – Occasionally, including Trigeminal Neuralgia
Balance and coordination impairment
Muscle weakness
Dizziness and vertigo
Vision problems, including double vision and downward nystagmus
Reduced gag reflex and dysphagia (difficulty swallowing)
Tinnitus (ringing in the ears) and hearing loss
Nausea and vomiting
Paralysis
In more severe cases, non-epiform seizures have also been documented
In addition to producing significant pain and neurological symptoms, the compression and kinking of the brain stem can cause significant injury to the brain stem neurons by stretching the axons of the nerves to the point that they break and recoil, producing what are called “axon retraction bulbs” that can be seen on microscopic examination of the cells. The stress placed on the brain stem by both compressing and stretching simultaneously is much greater than the mere sum of these two mechanisms. Interestingly, during the flexion of the normal spine, it stretches 17% of its length. Research has shown that the axon of a giant squid fails when stretched to 20% if its length. Therefore, the normal motion of the human neck brings us very close to injuring our brain stem. Consequently, it only takes a slight alteration of our normal anatomy to cause injury to these delicate nervous tissues[16].
Treatment of Craniocervical Instability typically begins with more conservative medical management, such as neck bracing, activity limitation, physical therapy (including isometrics, sagittal balance, core strengthening and cardio), and pain management. Other causes of symptoms such as co-morbid conditions, multiple sclerosis, dystrophy, mitochondrial disorders, vitamin deficiencies and Lyme disease should be ruled out or treated. However, surgical intervention via a craniocervical fusion is indicated when the following criteria are met:
Severe headache or neck pain >7/10
AND cervicomedullary syndrome
AND neurological deficits referable to the craniocervical junction
AND radiological findings indicative of instability
Surgeons and patients alike should consider surgery after medical management has been maximized and the patient has shown a positive response to neck bracing[10].
Various specific surgical techniques are applied in craniocervical fusions. A more common technique is the open reduction and fusion stabilization procedure. This procedure involves stabilizing the head with screws, making an incision that exposes the occiput through C2, and fixing plates to the occiput which attach to the C1 and C2 (and sometimes C3) vertebrae with rods. A newer technique adapted by Dr. Paolo Bolognese is using a less invasive Chiari decompression surgery known as MIST (minimally invasive subpial tonsillectomy) along with a fusion using screws placed in the occipital condyles. Although the dura is opened to partially resect the tonsils, a duraplasty is not done. Advantages of this procedure include a smaller incision, smaller hardware, less bone removal, and a thicker bone for which to insert screws in the occiput. Risks of both methods include vertebral artery injury, and a slightly increased risk for segmental instability below the fusion, along with the standard risks of any surgical procedure, such as bleeding, infection, and complications from anesthesia. Both procedures demand the hands of a very skilled and experienced surgeon because vital structures lie in and around the area. Using condylar screws may increase the risk of injury to major vessels, particularly in the hands of a less experienced surgeon. An important cranial nerve also lies just deep to the occipital condyles, making precise screw placement extremely important. This may limit the procedure in becoming more widely used, but the resulting fusion may be stronger, despite the reduced amount of hardware[17].
In the presence of a retroflexed odontoid, an open reduction, fusion and stabilization procedure may be enough to relieve ventral brain stem compression. However, in more severe cases, a further surgery called an odontoidectomy may be needed to remove the odontoid process. This surgery may be done through the mouth or the nose[18].
Every Chiari patient should be aware of hereditary connective tissue disorders and the signs and symptoms of Craniocervical Instability and Basilar Invagination. Many neurosurgeons do not evaluate their patients for these conditions prior to performing Chiari decompression surgery, often resulting in the need for revision surgeries and poor results. Being an educated patient can help you ask the right questions and insist on the proper evaluation and testing to avoid the pitfalls that many other patients have faced.
1 Bolognese, Paolo A, director. Surgical Techniques for Chiari Malformations. YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtu.be/KfYmJnB6sPQ>.
2 Bolognese, Paolo A. “Modern Classification and Subclassification of Chiari Malformations.”YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtu.be/ZQ9ZmquN-M0>.
3 Bolognese, Paolo A. “2016 ASAP CM/SM Conference – ‘Complex Posterior Fossa’ – Bolognese.” YouTube, American Syringomyelia Chiari Alliance Project, 7 Dec. 2016, <www.youtu.be/3jKH_DHadO8>.
4 Augustus A. White III, Manohar M. Panjabi, et al. “Clinical Biomechanics of the Spine.” By Augustus A. White III, <www.leomed.at/listhoscan/white_90.pdf>
5 The Pain Relief Foundation, The Pain Relief Foundation, <www.thepainrelieffoundation.com/craniocervical-instability/>.
7 Menezes, Arnold H. “Craniovertebral Junction Anomalies: Diagnosis and Management.”Seminars in Pediatric Neurology, vol. 4, no. 3, Sept. 1997, <www.sempedneurjnl.com/article/S1071-9091(97)80038-1/fulltext>.
8 Yang, Sun Y., et al. “A Review of the Diagnosis and Treatment of Atlantoaxial Dislocations.”Global Spine Journal, Georg Thieme Verlag KG, Aug. 2014, <www.ncbi.nlm.nih.gov/pmc/articles/PMC4111952/>.
9 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
10 Henderson, Sr. , Fraser C. “Neurological Management of Hereditary Disoders of Hypermobility Connective Tissue Disorders.” Ehlers-Danlos Society Annual Conference 2015. Ehlers-Danlos Society Annual Conference 2015, 14 Aug. 2015, Baltimore, <www.ehlers-danlos.com/2015-annual-conference-files/Henderson_0.pdf>.
11 Hain, Timothy C. “Basilar Invagination, Basilar Impression and Atlantoaxial Subluxation.”Basilar Invagination, Basilar Impression and Atlantoaxial Subluxation, 19 Apr. 2013, <https://dizziness-and-balance.com/disorders/central/cerebellar/basilar_invagination.htm>.
12 Kim, Louis J., et al. “JNS JOURNAL OF Neurosurgery OFFICIAL JOURNALS OF THE AANS since 1944.” Treatment of Basilar Invagination Associated with Chiari I Malformations in the Pediatric Population: Cervical Reduction and Posterior Occipitocervical Fusion | Journal of Neurosurgery: Pediatrics, Vol 101, No 2, Nov. 2004, <www.thejns.org/doi/abs/10.3171/ped.2004.101.2.0189?url_ver=Z39.88-2003&rfr_id=ori%3Arid%3Acrossref.org&rfr_dat=cr_pub%3Dpubmed>.
13 Henderson, Sr. , Fraser C. “Cranio-Cervical Instability in Patients with Hypermobility Connective Disorders.” OMICS International, OMICS International, 18 Apr. 2016, <www.omicsgroup.org/journals/craniocervical-instability-in-patients-with-hypermobility-connective-disorders-2165-7939-1000299.php?aid=71754#11>.
14 Bono, C M, et al. “Measurement Techniques for Upper Cervical Spine Injuries: Consensus Statement of the Spine Trauma Study Group.” Spine., U.S. National Library of Medicine, 1 Mar. 2007, <www.ncbi.nlm.nih.gov/pubmed/17334296>.
15 Henderson, Sr. , Fraser C. “Diagnosis and Treatment of Craniocervical Instability in the Chiari Patient.” Chiari and Syringomyelia Foundation Educational Lecture. 20 July 2011, Greater Metropolitan Washington Area, Greater Metropolitan Washington Area, <www.youtu.be/U33T8JFXvk0>.
16 Henderson, F C, et al. “Neuropathology of the Brainstem and Spinal Cord in End Stage Rheumatoid Arthritis: Implications for Treatment.” Annals of the Rheumatic Diseases, U.S. National Library of Medicine, Sept. 1993, <www.ncbi.nlm.nih.gov/pmc/articles/PMC1005138/>.
17 Bolognese, Paolo A. “Surgical Techniques for Chiari Malformations.” YouTube, American Syringomyelia Chiari Alliance Project, 16 Mar. 2015, <www.youtube.com/watch?v=KfYmJnB6sPQ>.
18 Hwang, Steven W., et al. “C1–C2 Arthrodesis after Transoral Odontoidectomy and Suboccipital Craniectomy for Ventral Brain Stem Compression in Chiari I Patients.”European Spine Journal, Springer-Verlag, Sept. 2008, <www.ncbi.nlm.nih.gov/pmc/articles/PMC2527411/>.
![The Important Questions to Ask Your Neurosurgeon [Revised]](https://staging.chiaribridges.org/wp-content/uploads/2023/09/MRI-doctor_AS505903501.jpg)

![Overview: Chiari Comorbidities & Etiological/Pathological Cofactors [Revised]](https://staging.chiaribridges.org/wp-content/uploads/2020/12/DominoEffect_AdobeStock_107422335-copy.jpg)



 Today is 11th April, 2019. Spring is in the air, yet I struggle to appreciate its presence. My daughters are at school, my son is at home in bed yet again. Like so many other days he is unable to get up. My son is 19 years old and looks just like any other 19 year old. You would never guess that this 19 year old is fighting a tremendously unfair battle every single day and has done so for several years.
Today is 11th April, 2019. Spring is in the air, yet I struggle to appreciate its presence. My daughters are at school, my son is at home in bed yet again. Like so many other days he is unable to get up. My son is 19 years old and looks just like any other 19 year old. You would never guess that this 19 year old is fighting a tremendously unfair battle every single day and has done so for several years. I started carrying out my own research, which clarified the distinct link between brain disorders and compromised immune/digestive systems. Whereas his doctors are reluctant to make that link, the evidence is clear. 18 months after surgery, my son got struck down by glandular fever. Again, we were hopeful that this would only be a temporary setback. Today however, my son suffers from chronic fatigue syndrome as well as dysautonomia.
I started carrying out my own research, which clarified the distinct link between brain disorders and compromised immune/digestive systems. Whereas his doctors are reluctant to make that link, the evidence is clear. 18 months after surgery, my son got struck down by glandular fever. Again, we were hopeful that this would only be a temporary setback. Today however, my son suffers from chronic fatigue syndrome as well as dysautonomia. My son is my hero. My son is a fighter. My son has generally done what health professionals told him to do, taken every medication health professionals told him to take, followed the advice health professionals told him to take, yet the system continues to let him down. When I look into my son’s eyes, I still see this steadfast determination but I now also see pain and disillusionment. My son believed me when I told him we would overcome this together. My son believed me when I told him the worst would be over soon. My son doesn’t believe me anymore. I feel that I have failed him.
My son is my hero. My son is a fighter. My son has generally done what health professionals told him to do, taken every medication health professionals told him to take, followed the advice health professionals told him to take, yet the system continues to let him down. When I look into my son’s eyes, I still see this steadfast determination but I now also see pain and disillusionment. My son believed me when I told him we would overcome this together. My son believed me when I told him the worst would be over soon. My son doesn’t believe me anymore. I feel that I have failed him.
 But to look at the full history of what became known as a Chiari Malformation, we can begin by looking at the research of a German pathologist, named Theodor Langhans. In his research in 1881 (a decade before Hans Chiari conducted his research on what became known as a Chiari Malformation), while looking at syringomyelia (“a cavity created in the spinal cord”), he noted a “change in the cerebellar cavity.” Upon dissection of the cerebellum, he described the cerebellar tonsils as “two symmetrical pyramidal tumors,” pushing the brainstem forward.
But to look at the full history of what became known as a Chiari Malformation, we can begin by looking at the research of a German pathologist, named Theodor Langhans. In his research in 1881 (a decade before Hans Chiari conducted his research on what became known as a Chiari Malformation), while looking at syringomyelia (“a cavity created in the spinal cord”), he noted a “change in the cerebellar cavity.” Upon dissection of the cerebellum, he described the cerebellar tonsils as “two symmetrical pyramidal tumors,” pushing the brainstem forward. Unfortunately it leaves most of us with failed decompressions, fighting with our neurosurgeons that “something is still wrong.” These neurosurgeons look at their post-operative checklist and see that they successfully did everything surgically required in their out-of-date textbooks:
Unfortunately it leaves most of us with failed decompressions, fighting with our neurosurgeons that “something is still wrong.” These neurosurgeons look at their post-operative checklist and see that they successfully did everything surgically required in their out-of-date textbooks: