Most Chiarians go to see a surgeon with an expectation of them being knowledgeable in their field. However, while they might be a neurosurgeon, their knowledge of Chiari and its comorbid/pathological conditions might not rank high in their practice. Make the most of your initial appointment by interviewing them and what they really know about Chiari Malformations. Be cautious of inflated success rates. Chiari decompression in general offers a just over a 50% success rate (which means it has a nearly 50% failure rate). Surgeons that claim a 100% (or near 100% success rate) are usually not basing their success on how their patients feel afterward, it is based on if they were successful with the aspects of the surgery: Removal of the occipital bone ✓ Opening the dura and adding the patch/graft ✓ Laminectomy ✓ Cauterization/resection of cerebellar tonsils ✓
WE DESERVE BETTER THAN THAT!
HERE IS A LIST OF CHIARI QUESTIONS WE RECOMMEND ASKING AT YOUR FIRST NEUROSURGERY APPOINTMENT:
General Questions:
How do you define a Chiari Malformation?
What do you believe causes a Chiari malformation?
Are all Chiari malformations from a small posterior fossa?
Do I have a small posterior fossa? If yes, how big is it? If size is unknown, was my posterior fossa measured? If not, why not? How did you come to the conclusion that I have a small posterior fossa?
How common do you believe Acquired Chiari malformations to be?
Do you always recommend decompression surgery for all of your patients with herniated cerebellar tonsils? Why/why not?
In an average month, how many Chiari decompressions do you perform? How many tethered cord releases? How many craniocervical fusions? What percentage of your practice is spent treating patients with these connective tissue related conditions?
Looking at my brain scan, is any part of my “brainstem” herniated (below the posterior fossa)? If so, does that make me a Chiari 1.5?
Intracranial Hypotension (low pressure) Questions: *Article to help you understand CSF Leaks & Intracranial Hypotension prior to your appointment. If you have SYMPTOMS OF LOW INTRACRANIAL PRESSURE and/or suspect a cerebrospinal fluid leak, we recommend asking the following questions:
S.E.E.P.S.
Looking at my brain scan, do you see any Subdural fluid collections?
Looking at my brain scan, do you see an Enhancement of pachymeninges?
Looking at my brain scan, do you see an Engorgement of my venous structures? Should we do an MRV to make sure?
Looking at my brain scan, does my Pituitary appear to be enlarged?
Looking at my brain scan, does my brain appear to be Sagging?
Looking at my corpus callosum:
Does there appear to be a depression?
Is there an inferior pointing of the splenium?
If he/she answers affirmatively to any of the above S.E.E.P.S. questions, ask:
What should be done to find/repair a potential leak?
Are you aware that it is common for CSF Leaks to not show up on MRI?
Are you willing to do a CT Myelogram and/or a digital subtraction myelogram, if I develop symptoms of a leak and none can be found on MRI?
Are you aware that it can often take multiple epidural blood patches to try and seal a leak, and sometimes when a blood patch fails to work, a surgical dural repair might be necessary?
Intracranial Hypertension (high pressure) Questions: *Article to help you understand Intracranial Hypertension prior to your appointment. If you have SYMPTOMS OF HIGH INTRACRANIAL PRESSURE, we recommend asking the following questions:
Looking at my brain scan, do I have cerebrospinal fluid in my sella turcica (Empty Sella Syndrome)?
Looking at my brain scan, do you see any evidence of my optic nerves are swollen (papilledema)?
If so, should I be referred to a neuro-ophthalmologist?
Looking at my brain scan, do my lateral ventricles appear small or flattened?
If so, do I need to have my pressures checked?
If yes, are you aware of the risks of developing a CSF Leak from a lumbar puncture?
What are the symptoms of a CSF Leak, should one develop?
What is your plan of action if I should develop these leak symptoms?
Are you aware that it is common for CSF Leaks to not show up on MRI?
Are you willing to do a CT Myelogram if I develop symptoms of a leak, and none can be found on MRI?
Should a leak be found, are you aware that it can often take multiple epidural blood patches to try and seal a leak?
Tethered Cord Questions: *Article to help you understand Tethered Cord: Sorry, Coming Soon. If you have SYMPTOMS OF TETHERED CORD, we recommend asking the following questions:
Looking at my brain/cervical scan, does my brainstem appear to be elongated?
Looking at my cervical scan, does my spinal cord appear to be stretched?
Looking at my lumbar scan, does my conus reach my mid/low L2?
Looking at my thoracic and lumbar scan, does my spinal cord appear to be pulling to the back, or one particular side?
If so, should we do a prone MRI to see if it has actually adhered to that side?
Looking at my lumbar scan, do I appear to have fatty tissue inside the epidermis?
If the answer to any of these questions is affirmative, do you suspect that I have a tethered spinal cord?
If so, should we plan for a Tethered Cord Release before or soon after decompression surgery, so the likelihood of a failed decompression is reduced?
If I have urological issues, can I get a referral for urodynamic testing to rule out any other potential causes of my urological issues?
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI): *Article to help you understand CCI & AAI prior to your appointment. If you have SYMPTOMS OF CRANIOCERVICAL INSTABILITY or SYMPTOMS OF ATLANTOAXIAL INSTABILITY, we recommend asking the following questions:
Looking at my brain/cervical scans, what are the measurements of my clivoaxial angle and Grabb-Oakes?
Do these measurements meet the diagnostic criteria for Craniocervical Instability?
Looking at my flexion and extension imaging, how many millimeters of translation are there between flexion and extension?
Does Chamberlain’s Line cross my odontoid? If so, does it cross at a level that would indicate Basilar Invagination?
Looking at my rotational imaging, what is the percentage of uncovering of the right and left articular facets on rotation?
Do the percentages from my rotational imaging meet the diagnosis criteria for Atlantoaxial Instability?
IF A DIAGNOSIS CRITERIA IS MET IN ANY OF THE ABOVE, WE STRONGLY RECOMMEND THAT YOU WAIT ON DECOMPRESSION AND PURSUE THE TREATMENT OF SAID CONDITION(S) AND THAT OF EHLERS-DANLOS SYNDROME, AS EACH OF THESE CONDITIONS CAN BE PATHOLOGICAL TO AN ACQUIRED CHIARI AND EACH IS A STRONG INDICATOR THAT A CONNECTIVE TISSUE PROBLEM EXISTS.
*The questions in this article will periodically change as we are able to expand our recommended questions.
*Original version released September 2018, revised 2023.
As I sit down to update my journey, I am crushed that we’re still figuring things out (and nothing really was as I was initially told it would be), yet at the same time, I’m so thankful that we’re continuing to figure things out. Nobody should have to fight a fight like this (every symptom, every diagnosis), but all of this just increases my resolve to change it before anyone else in my family (or yours) is having to fight it! What we fail to change in our generation, our children and their children will face in theirs!
Looking back, I have always had symptoms of Ehlers-Danlos Syndrome (EDS). As a child, I was in the school nurse’s office for stomach problems at least once a week. I was “double-jointed” and my friends always asked me to do maneuvers that I thought everyone should really be able to do if they tried. I was athletic early on, a tom-boy. I particularly loved playing softball (or baseball with tennis balls was the absolute best), but my ankles rolled when I started to run. Despite the fact that I was the only player that twisted their ankle multiple times in every game, I didn’t think there was really anything abnormal about me. Later, as an adult, I had repeated miscarriages and complications in all of my pregnancies, but the doctors conveniently came up with different explanations for each “rare occurrence.” It couldn’t possibly be all those rare mishaps, but EDS explained it all.
My mother passed away from a brain aneurysm the day after my 18th birthday. She was just 37 years old when she died. As a child she had a lazy eye and scoliosis of the spine, so an eye patch and back brace were a normal part of her childhood attire. She suffered from migraines throughout her adulthood, but nothing was more tale-telling than reading her journal after she passed, with multiple entries about repeated headaches and neck pain. Decades after her death, my maternal grandmother (my mother’s mother) developed multiple brain aneurysms over the course of a decade. Each time one appeared, she had it filled with titanium coils. I always admired her fight for life.
Me and my mom (1971).
The first headaches that I remember started immediately after giving birth to my first son in 1992. It was a cesarean section at an Army hospital in Fort Ord, California. Instead of an epidural, they gave me three spinal injections to numb me from the chest down. At my postpartum check-up, I complained of daily headaches when upright. My primary care doctor ordered a CT scan, but because it was just a few years after my mom had died they looked only for brain aneurysms and found none. I was still having those orthostatic headaches six months later.
Me and my eldest son, Johnathan (1992).
The Accident that Shook Everything
In 2000, I was a Bible College student and stay-at-home mom of three happy and active children (ages 8, 5, and 2). One September night, I was in a car accident that changed all of our lives. My neck was never the same again. My initial symptoms were head/neck pain, but all radiology reports indicated that everything was “unremarkable.” I tried everything they offered to me: rest, acupuncture, acupressure, steroid injections, osteopathic and chiropractic care, nerve stimulation units, physical therapy, pain meds, etc. Nothing worked long-term. Then in 2005, my neurological problems started intensifying. I began having bouts of partial paralysis in my legs and hands. I would just wake up one morning and out of the blue, I would have no fine motor skills. I would wake up feeling as though I had no thigh muscles to support me when I walked or tried to step up a step, and I had difficulty coordinating my footsteps. My primary care doctor at the time did blood tests and concluded that my “potassium level was on the low side of normal, so it must have been from potassium shock,” and he thought that no other tests were warranted. I started having vertigo whenever I was at any elevated height, even just a step or two up, like my brain couldn’t figure out how to balance with visual changes in height (I’d take a step up or down like the step was much higher or lower than it actually was). I also started having noticeable memory issues and intermittent trouble processing information. They tested to see if I was having small seizures in my sleep. When that was ruled out, they referred me to the memory clinic for further cognitive testing. They had no cognitive baseline to compare my results to, but said that I “tested higher than 89% of the population, so I should be happy,” and that I should just try reducing stress in case it was stress-related. They didn’t understand that it didn’t matter to me “how I compared to others.” I was only 34 years old and something was very wrong with me; I wanted answers that had nothing to do with the general population. In 2006, my eyes started twitching all day, every day, until the muscles just wore out and I could no longer hold them open completely. Oddly, one of my college professors inquired about my eyes and recommended that I have it investigated because it “could be neurological in origin.” When I did talk to my doctor about it, he saw the recommendations of the Memory Clinic and attributed it to stress as well, without any testing.
My Chiari Diagnosis
Finally, in 2010, ten years after the car accident, another MRI was done at my insistence to check for aneurysms once again (because I still was having excruciating head/neck pain and trouble holding my head up). I received an email from my primary care doctor that they found a cause of all of my symptoms. It was a condition called Chiari Malformation and the neurosurgery department would be contacting me to make an appointment. The neurosurgeon (who became my neurosurgeon) checked through my MRIs and said that the Chiari Malformation was evident on my first MRI after the accident ten years earlier. I was told that it was congenital and that it is commonly believed to be a result of prenatal drug use or lack of proper prenatal care (which was devastating to hear, but not all that unlikely as I was born in 1971. It also ended up being very wrong “textbook information” that they tell us all). Desperate for a measure of relief, I underwent a full decompression surgery a few weeks later. Missing the fact that part of my brain was in my spinal canal was 100% the hospital’s fault, but in hindsight, I really wish that I had done more research before surgery. I had comorbid conditions (many of which my doctors hadn’t even heard of, didn’t fully understand, and more importantly, they didn’t know the connection between these comorbids and my herniated tonsils). Initially, I felt quite a bit better. The release of pressure in my head helped my headaches. It was short lived though. Those undiagnosed comorbids caused my decompression to ultimately fail, although it all unfolded over several years.
My preoperative MRI (2010).
Post-op Complication: Pseudomeningocele
When I was released from the hospital following decompression surgery, I was instructed not to lift, push, or pull anything for two weeks so that my dura patch would have a chance to adhere. The problem was, I could feel fluid squeezing out of the patch far beyond that two-week limit. I developed a pseudomeningocele (blue box above), which can be normal immediately after surgery before the dura adheres, but as long as there is no active leak, the body should absorb the fluid and the pseudomeningocele should quickly resolve. My neurosurgeon tapped some of the fluid out with a syringe twice and we waited patiently to see if it would subside on its own. It did not subside and in December 2012 (just over two years post-decompression), I developed acute vertigo. Everything was spinning and rocking, non-stop. It didn’t matter if my eyes were open or closed. I was waking up vomiting in my sleep from the dizziness. I couldn’t walk at all without falling hard to my right. I had no sense of balance at all and it didn’t just come and go, it was constant. Another MRI was done and it showed that my cerebellum was absorbing the fluid from the pseudomeningocele (so the cerebrospinal fluid was inside my brain, not just surrounding it; see light blue circle in image above). The decision was made to put in a subgaleo-peritoneal shunt (SP shunt), which runs from the pseudomeningocele to my peritoneum. They expected that it might take up to six months to fully drain from my cerebellum, but I woke up from the anesthesia with no signs of vertigo. I believe this surgery saved my life, but as with all shunts (especially amongst those with EDS, which I had not yet been diagnosed with), the shunt was destined to cause problems all by itself.
Postoperative MRI (2012)
My Many Shunt Revisions
In April 2013, an unrelated CT Scan revealed that my shunt was no longer in my peritoneum. My NS scheduled for a general surgeon to “tie in” my shunt so it would not happen again (surgery #3). We went several months without complication until that November. The tied in shunt pulled out of my peritoneum again (it was excruciating). Hoping gravity would help in the matter, my NS did an incision just under my right rib cage and dropped it down into my peritoneum (surgery #4). Shortly thereafter, radiologist reports started showing a concern for the location of my brain and I was diagnosed with “Sagging Brain Syndrome.” So my six-week post-op appointment (which my NS did faithfully after every surgery) became my pre-op appointment for my 5th related surgery. This time a non-adjustable valve was attached to the shunt (at my chest) in hopes that by slowing down the amount of CSF being drained by the shunt, my head could retain more fluid and my brain could once again lift and become buoyant. Five months later I developed a hernia and upon closer examination (during surgery), it was found that my peritoneum was literally falling apart from all the trauma of the shunts; so my hernia removal surgery became a reconstruction surgery where my abdominal wall was pulled together with mesh, while carefully ensuring that the shunt didn’t come out (surgery #6). The shunt never moved again. As my brain continued to sag, the choice was made to replace the valve with an adjustable valve and in November of that same year, I was having surgery #7. The valve was adjusted to its slowest possible setting in hopes of finding a balance where it drained enough to keep the hydrocephalus at bay, yet retain enough CSF to lift my brain and keep it lifted and out of my spinal canal (so we could establish flow to the spinal canal and avoid the possibility of a syrinx).
Diagnosis: Ehlers-Danlos Syndrome
Despite my concerns that I might have a connective tissue issue and being told over-and-over again that I “didn’t look like someone with Ehlers-Danlos Syndrome,” I was finally diagnosed with it in May 2015. After finally finding a neurologist who understood the role that our connective tissues can have in a Chiari Malformation, I was given a referral to a geneticist. It still wasn’t as easy as it should be though. The geneticist did not know much about Chiari or Ehlers-Danlos related conditions (although he didn’t initially admit to that), so I had no idea at that point what was and was not related, and neither did my doctors. I received a call from the geneticist’s assistant and I agreed to send her pictures of my hypermobile maneuvers from the Beighton Scale. I could do all but bend over and put my hands flat on the floor with my knees straight, but I was able to do that when I was younger (and thinner). I was given a 9/9 on the Beighton Scale and was told that he would just mark my chart as diagnosed “hypermobile” and that he didn’t need to see me. I honestly didn’t know any better at this point, but I was about to learn something very important. I sat there thinking about what this “hypermobile” diagnosis would mean for me and decided to look more into EDS for myself. I read about the high risk of aneurysms, organ tearing, miscarriages, etc. and I was back on the phone with that assistant within twenty minutes. She asked if she could call me back, and within the hour the geneticist had decided that he needed to see me. He set up an appointment with me within twenty-four hours and asked if it was okay if he had a few others (doctors and medical students) there as well, since they’re a training hospital and they “don’t really come across patients with Ehlers-Danlos” (he should have told me that from the beginning). I agreed. Despite his lack of knowledge on EDS related comorbidities, he did know exactly where on my body to look for characteristics of EDS (all of which I thought I didn’t have). For instance, my skin isn’t unusually elastic, except in my upper arms and upper thighs. My skin isn’t translucent (I’m olive complected), except for on my breasts, back, and inner forearms. My skin isn’t unusually soft, except on my back. Now concerned that I might have Vascular Type EDS (vEDS), he decided to have me tested for that. The test was easy on my part but expensive on theirs. They drew blood and had it refrigerated and shipped to a lab in Washington state. It took thirty days for them to make sure that there was no mutation in my COL3A1 (collagen 3; alpha 1) gene, which has a median mortality age of 48. Initially, I felt devastated, since I was already 44. I decided that I hadn’t fought through all that I had, to only live a few more years. Thirty days later, the test came back indicating that I didn’t have vEDS and by default, I was diagnosed with Hypermobility Type EDS (hEDS). I was relieved, but the geneticist assured me that I still needed to be cautious. Since EDS symptoms are known to cross the type boundaries, and we already knew that vascular complications ran in the family (with the aneurysms) and with me personally (my peritoneum tearing), it technically made me “hEDS with vEDS crossover symptoms” and I’d probably have to explain that to my doctors for the rest of my life, so they remain aware of my potential to have additional vascular problems.
My Poor Mess of a Neck
The electric shock feeling in my spine (Lhermitte’s Sign) that I’d had intermittently for years, became an all-day, everyday thing, and much stronger in intensity. The MRI revealed that the herniated disc I had between my C3/4 was getting worse. The disc was removed with cadaver put in its place and the discs were fused together. My 8th surgery (ACDF = Anterior Cervical Discectomy and Fusion) wasn’t related to Chiari, but it was related to the EDS. We knew that my cervical spine was really bad from the beginning, but it got worse. I am now actually diagnosed with Degenerative Disc Disease in all three levels of my spine, but my neck has by far taken the brunt of it all. The ACDF, while 100% necessary, compromised the discs adjacent to it, and every disc from C4-7 is either bulging or herniated (Subaxial (cervical) Instability), so additional surgeries are likely to be needed.
Learning to Advocate for Myself
Over the past several years I have become an enthusiast of Chiari related research and MRIs (out of medical necessity more than anything). It became apparent to me that I absolutely needed to know everything that was going on in my body in case my doctors didn’t. When I first started, I’d print out studies and lay in bed with multiple high-lighters. I had such brain fog that I’d lay there crying at the fact that I was reading and rereading the same paragraphs over again, but I knew that I had to learn it despite how impossible it seemed. I prayed a lot for God to help me with my understanding and He did. I also started looking at the medications I was taking, the supplements I was taking, and what the ideal doses were for me (especially those that would help with inflammation and cognition), and other natural remedies. The first thing that I removed was all of the nerve meds that they had me on for peripheral neuropathy. I was maxed out on Nortriptyline (a tricyclic antidepressant) and almost maxed on Gabapentin (both of which had caused me to gain an incredible amount of weight over the years). When I informed my primary care doctor that I wanted to go off of them all, he thought it was a bad idea because of the severity of my neuropathy. I insisted though and asked him to help me to wean myself off of both of them in healthy intervals, and let’s “just see.” With the first down-dose, I physically felt a reduction in inflammation. It took me many months to wean off and get them out of my system, but in hindsight, I think this was the single best decision that I could have made. The longer I was on supplements instead of the nerve meds, the more my brain-fog improved, and I now believe that I have regained all that I’ve lost cognitively and then some.
Syringobulbia
In 2016, I was reviewing some of my old MRIs and I saw a large CSF filled hole in my lower medulla oblongata (lower brainstem). It was obvious in all MRI series since 2015, yet I was told that all was stable. After researching it, I asked my neurologist to take a look and see if it could be Syringobulbia. She referred my question to my neurosurgeon and he confirmed that I had an 11mm cyst in my brain stem. This type of cyst happens when there is a blockage of cerebrospinal fluid and is most frequent when the brain stem is also herniated below the foramen magnum (Chiari 1.5). It explained a lot of the problems that I was having, that we had thought to be unrelated. For instance, and I had a decreased sensitivity to temperature for years, never feeling hot or cold; and never having the automatic reactions that I should have had in response to temperature, like sweating and shivering. I could comfortably be outside in heat above 100° without breaking a sweat, or be outside in shorts and a tank-top when it was a chilly 30° morning without ever shivering. I also developed tachycardia and I am now medicated to keep my heart rate down to a safe level. My neurosurgeon ordered a new MRI in April 2017. The size of the syrinx had decreased to 9mm but was draining down my spinal cord forming an additional syrinx (Syringomyelia).
Syringobulbia. Left – Syrinx in 2015 measuring 11mm in diameter. Right – Syrinx in 2017 measuring 9mm in diameter.
Consulting a Specialist
After all that I had been through in my fight, in April 2017, I decided to pay out of the pocket and have an online consultation with a Chiari Specialist in New York, who specializes in Chiari with EDS (the best $300 that I’ve spent in my fight). I sent him my pertinent medical records and copies of my MRIs in advance, wanting to find out what my doctor did right, and what he did wrong; and what course of action should be taken at that point. My expectation was that he would give me reasons why I should go to New York to see him, but that’s not at all what he told me. He told me what my doctor did right and that he didn’t disagree with the course of action that my neurosurgeon wanted to take. He said that my brain had sagged as low as it really could, but that since my high/low pressures had balanced out, and I was feeling better than I had in years, my syringes really should dictate our next course of action.
In March 2018, following an exceptional year (at least where my head and neck are concerned) new imaging was done. My neurosurgeon asked me to come in to review it. It gave me a chance to tell him about the specialist’s opinions. My MRI showed that the Syringobulbia had decreased another 2mm. I asked him what that meant for the cervical syrinx, and that had almost completely disappeared. I asked him to go back to my images and correct me if I was wrong, but “the only reason that a syrinx (in either location) would dissipate like that was if I was finally getting CSF flow down my canal (despite my severe brain sag).” He agreed and I think he was a little surprised to see me think on my feet and figure that out in front of him (where I wasn’t having to ask anyone or look it up). He also confirmed that I had an Acquired Chiari, secondary to Intracranial Hypertension. He applauded me for learning all that I had and said that he wished that he had checked my pressures before decompressing me, as it may have changed the course of action that we had taken. And we agreed to wait a year and see where the syringes (syrinxes) are. As I left his office that day, I felt such a sense of relief, that we were finally getting CSF flow like the decompression in 2010 was meant to do.
My Extensive Epidural CSF Collection
In 2022, my neurosurgeon contacted me telling me that he was retiring and he’d like to have one last MRI of my entire spine (he added the brain to the request at my request). Unbeknownst to me, he ordered a CSF Leak Protocol, which consists of less slices, but they’re specifically looking for leaks. The images showed an “extensive extradural CSF collection from C7-L4, consistent with a CSF Leak and probable dural tear or CSF Venous Fistula.” They followed up with a Dynamic CT Myelogram. A Dynamic is different than a regular CT Myelogram, as they do it over 2-3 days, and they insert the contrast little by little into my spinal canal, and watch carefully for it to leave the spinal canal. CSF leaks and dural tears aren’t uncommon amongst Ehlers-Danlos patients, and usually happen in the front or back of the canal. CSF Venous Fistulas on the other hand are a much newer phenomenon, and they usually happen on the sides of the canal (more often on the right side). After two days of grueling tests, they found no active leaks or evidence of fistulas and surmised that what they saw on the MRIs to be “residual artifacts” from a leak that I had in the past… a leak that could have pulled my brain down into my spinal canal in the first place.
Sagittal and axial views of my thoracic and lumbar images showing the residual artifacts of an extensive extradural CSF collection.
It’s been a long road, hard road. I still battle inflammation and I’m definitely not done with surgeries. Eventually, I will need a ventriculoatrial (VA) shunt to hopefully resolve my high-pressure issues and enable us to remove my over-draining SP shunt that is making my brain sag. But for right now, I’m just enjoying feeling so much better! I praise God every step of the way, as I know that He’s there making a way out of no way. I have no idea why He took so long or why others haven’t seen the same results (because He loves them as much as He loves me), but I don’t have to have all the answers. I’ll just praise Him through the course of my journey, as He’s never let me go through it alone!
*I dedicate this story to my family: John (husband), Ron (dad), Johnathan (son), MyKaella (daughter), Jojo (son) and my daughters-in-law, Violet and Sarah. Thank you all for all your help and for standing and kneeling beside me throughout my entire ordeal. You’ve been there for me and loved me through this long haul and I praise God for each and every one of you.
“But you look so good” is what people usually say when they find out that I struggle with debilitating chronic illnesses. It is true- I wear fashionable clothes, I do my hair, I put on makeup and I have a smile on my face. Underneath it all though, is someone who is trying to live her best life with the cards she was dealt with. I grew up in southern India and none of my family members knew what Chiari malformation was. It wasn’t until I came to the United States, had a baby and hit a complete rock bottom that I found out that a condition called Chiari even existed.
The journey to diagnosis was much like putting together a jigsaw puzzle especially when my medical providers did not take me seriously. The pain came first-it started in my fingers, head, neck, knees and gradually, over the course of two years became fairly debilitating. I was initially misdiagnosed with Rheumatoid arthritis since I have a family history with it. I was on sulfasalazine, prednisone, and hydroxychloroquine for over a year. While the prednisone helped with the pain, the combo of drugs just made me sicker and sicker. I went down to 95lbs and got extremely depressed. It was easy for everyone to simply say that I was homesick and that my pain was imagined. Yes, I was depressed but not due to homesickness. It was legitimate and severe pain that existed but could not be seen or measured by a test. I was sent to a psychologist and then to a psychiatrist. I was just “the immigrant who was dealing with immigrant-related depression and anxiety.” When multiple medical providers went with that same narrative, I started questioning if it was all indeed in my mind and psychosomatic. I was starting to accept that living like that was going to be my new normal. I was training with my figure skating coach to be able to make to adult nationals. Skating gave me joy because it was an artistic sport that I could distract myself with. But eventually, the pain took that joy away from me.
During this time, I became increasingly bitter and angry with everyone around me including my family members. I felt alone and invalidated over and over. In hindsight, I can understand why it was hard for my family to believe my pain too. No one knew about the monster that was causing it. Things got even weirder when I was pregnant- my body reacted negatively to pregnancy. I had gestational diabetes, polyhydramnios and mysteriously, two rib fractures that perplexed everyone. I was induced at 39 weeks with a labor that lasted over 30 hours and ended with fourth-degree external and internal tears. While my rib fractures and severe tears were a red flag, they were apparently not a red flag enough to warrant a deeper look at what was going on. It was still easier to stick to the hysterical, angry woman of color/ immigrant narrative. The physical scars from my fractures and tears healed and the emotional scars were temporarily masked by the joy of my new baby girl. Days turned into weeks into years and pain was my normal. Having no pain was a red flag at that point.
Slowly, my esophagus deteriorated, and my lower esophageal sphincter completely gave away. My nasal septum deteriorated somehow, I developed a near-constant tremor. People were starting to see some outward signs of what I had been complaining about for years. After a motor vehicle accident, my symptoms took a drastic turn for the worse. I had to fight with my primary care doctor to get an MRI. It took me 7 years at this point to learn that if I did not fight for myself, then no one would. And I wanted my baby girl to have a mom around.
From the diagnosis of Chiari 1.5 to surgery was about 3 weeks. I liked my surgeon and the care team, so I was comfortable with the surgery. Recovery was long and painful though. I had meningitis twice after the surgery, developed chronic migraines in addition to trigeminal and occipital neuralgia. The diagnosis of central sleep apnea, MCAS and EDS came a year later. My brain stem was traumatized massively. I had to go to vestibular physical rehabilitation therapy to fully walk independently again. A year after my Chiari decompression, I had the Nissen Fundoplication to fix my esophagus. Four years past surgery, I am still recovering and learning how to manage my conditions. My care team now consists of – Anesthesiologist, Physiatrist, Neurologist, Pulmonologist, Gastroenterologist, ENT doctor, Massage Therapists, and Mental Health Counselors in addition to my close family. A huge part of learning how to manage these conditions has been figuring out what my physical limitations are and listening to my body cues. It has taken a long time to learn that it is ok to say no and that it is ok to have a LOT of mental energy but have little to no capacity to do things physically. I gave up figure skating because that kind of physical activity was causing me extreme pain. I get intense urges to skate every now and then which I give into occasionally but as the years have gone by, I am much better at gauging the pain and deciding not to do it. Loud sounds and bright lights trigger a lot of pain now, so I am better about avoiding places that I know are noisy and overwhelming. I have found peace in hiking through the wonderful trails of the pacific northwest. I have cut down on social commitments to prioritize my health over anything else. Some weekends, I do nothing except sleep all day… I have had to learn that that is OK. My husband has been a huge support and my pillar to lean on for the 11 years that we have been married. If I am tempted to do something against my better judgment, he reminds me to know my limitations. I have made peace with the fact that some people might find it impossible to hard to understand what living with Chiari and the comorbid conditions is like and that I cannot control how other people see it. My job has been a stable and joyful part of my life, but it took me a long time to accept that too since my original goal was to go to medical school. I realized my personal limitation about not being able to make it through medical residency. I want to let everyone know that there is hope at the other end of the tunnel… even though it is not in the form of a cure.
INTRACRANIAL HYPERTENSION (IH) MEANS HIGH PRESSURE INSIDE THE SKULL.
Intracranial Pressure (ICP) is measured in millimeters of mercury (mmHg). Most scholars agree that on average, “normal pressure” should be between 5-15 mmHg, mild to moderate intracranial hypertension between 20-30 mmHg (which “requires treatment in most circumstances”), and an ICP of > 40 mmHg indicates “severe and possibly life-threatening intracranial hypertension.” [1] When high intracranial pressure is left untreated, it creates a “pushing effect” towards the only natural escape at the base of the skull (the foramen magnum), and the cerebellar tonsils in the pathway are pushed through the foramen magnum. [2]
Understanding the Monro-Kellie Doctrine (pressure-volume relationship) The association between IH/IIH and Chiari Malformation appears to be a malicious intricate pathological circle. The cranium (skull) consists of brain matter, cerebrospinal fluid, and both venous and arterial blood. A hypothesis, referred to as the Monro-Kellie Hypothesis (now better known as the Monro-Kellie Doctrine), states, “The sum of volumes of the brain, CSF, and intracranial blood is constant. An increase in one should cause a decrease in one or both of the remaining two.” Therefore, if an abundance of cerebrospinal fluid (IIH or hydrocephalus), both cranial blood volume and brain matter should be forced to deplete. This depletion is usually directed in the path of least resistance – through the foramen magnum and into the spinal canal. When the brain matter closest to the bottom of the skull (cerebellar tonsils) is pushed through the foramen magnum and into the spinal canal (an Acquired Chiari Malformation), the tonsils act like a cork and blocks the flow of cerebrospinal fluid (regardless of the size of the tonsillar descent), which in turn, continues to raise intracranial pressure.[3]
Venous Hypertension
When an etiological cofactor exists (such as a space-occupying mass), it is considered Secondary Intracranial Hypertension (SIH); when no other cause was identified, it is known as Idiopathic Intracranial Hypertension (IIH) formerly known as Pseudotumor Cerebri. However, recent studies on the connection between Intracranial Hypertension and Venous Hypertension might put an end to the “idiopathic” theory.
Oxygen-rich blood travels from the heart to the rest of the body through the arterial system, then the oxygen-depleted blood returns to the heart through the venous system. We have a host of small veins in our head and they dump into a series of large veins, called sinuses. Dural Venous Sinus Stenosis occurs when there is a narrowing of one or more of the venous sinuses (most commonly seen in the transverse sinuses or transverse/sigmoid sinus junction), which in turn compromises cerebral venous outflow through the jugular vein (stenosis/compression of the jugular vein can also result in elevated intracranial pressure [4]). Transverse Sinus Stenosis (TSS) is most common in Idiopathic Intracranial Hypertension (IIH). Depending on the study that you are reading, it is proving to be present in 90-100% of IIH patients [5]. While its connection might sound obscure if you look at it from a Monro-Kellie perspective – The blood going into the head, cannot get out at the same speed (because of the narrowed sinus). When this inflow of blood remains constant and the outflow is hindered, the transverse sinus on that side (we have two transverse sinuses, one on each side) enlarges, forcing the CSF and brain matter to reduce to maintain the volume equilibrium. This reciprocation can happen when any of the sinuses or jugular narrow (stenosis). While scholars continue to debate whether TSS is a cause or consequence of IIH, surgeons continue to decompress us without checking our pressures or decompress (the most invasive treatment) in hopes that it will lower our pressures, and patients are left with untreated high pressure still causing a “pushing down effect” and an enlarged foramen magnum for our brains to be pushed down. [2] The sagging brain once again obstructs the flow of cerebrospinal fluid by plugging the foramen magnum, and that in turn raises the intracranial pressure even more. Or, the untreated high pressure blows through the duraplasty and causes a post-operative leak, known as a pseudomeningocele.
Reducing the Risks of Post-Op IH/IIH Complications
Brain MRIs often show indicators of Intracranial Hypertension (IH/IIH), therefore, we recommend that all Chiari patients have full brain MRIs and not just cervical MRIs.
• When the pressure builds inside of the dura mater the pressure pushes the dura and fluid inside of the crevice that holds the pituitary gland (the sella turcica or pituitary fossa). When the amount of fluid is equal to or greater than 50% and the pituitary gland size is 2mm, the condition is known as Empty Sella Syndrome. (Doctors now recognize that < 50% (where the pituitary gland size is 3-7mm) can also cause symptoms and they now refer to that as a partially empty sella.) [8]
• Slit like or flattened lateral ventricles from the increased pressure, however, when the Foramen of Monro (the aqueduct that connects the lateral ventricle to the third ventricle) is stenosed, the fluid will back-up and the lateral ventricle will not appear flattened. [7]
• Low lying or herniated tonsils (often diagnosed as a Chiari Malformation). [2]
What We Recommend BEFORE DECOMPRESSION is considered:
If you have symptoms of IH/IIH accompanied by any of the MRI indicators mentioned above, it is both reasonable and prudent to ask your neurosurgeon to investigate further BEFORE DECOMPRESSION.
See a neuro-ophthalmologist to check for signs of papilledema, including Optical Coherence Tomography and Ultrasonographic B-scanning. [8]
Magnetic Resonance Venography (MRV, preferably with the ATECO technique) to check for venous stenosis of any of the cranial sinuses and/or jugular vein. Stenosis is not exclusive to the transverse sinus and it can happen in multiple sinuses simultaneously.
If overweight, consider trying to lose weight. Studies show that a weight loss of 5-10% of one’s overall body weight, when accompanied by a low-salt diet, can offer some to IH/IIH symptoms.[9]
Consider trying Diamox (Acetazolamide) and/or Topamax (Topiramate) to see if that improves the pressure headaches.
Request a lumbar puncture (spinal tap) to test your opening pressures. We recommend that it’s guided with fluoroscopy with a small gauge needle (and not the standard 22 gauge) that they allow to drip (as opposed to syringe pull) and ensure that someone is available to perform an epidural blood patch if necessary. Time should be allotted afterward to lay flat for several hours immediately following the procedure and for several days once returning home. The potential for CSF leaks is high for the EDS/Chiari patient. A doctor that marginalizes the risks ahead of time, will generally marginalize your symptoms when you are actively leaking.
ICP Bolt Monitoring can record the differences experienced in pressure over time, and how different positions affect ICP.
Note: When the intracranial pressure gets high enough, it can cause a cranial leak. This is especially true for the Ehlers-Danlos patient where the dura mater is thin and fragile. When a cranial leak decreases the intracranial pressure, the papilledema, empty sella, stenosis, and high-pressure headaches can sometimes start to revert to normal or near-normal, and the leak will affect any attempts to check intracranial pressure (reducing the pressure from what it was before the leak occurred), however, the tonsillar herniation will usually remain if the pressure gets too low. [10]
TREATMENT OPTIONS:
If Venous Stenosis exists, stenting should be considered as leaving the sinus/jugular stenosed can post other health risks, and stenting is proving to have much better success with fewer complications requiring revisions. When medication fails to decrease ICP, and a stent is not an option, a Ventriculoperitoneal Shunt (VP Shunt) or Ventriculoatrial Shunt (VA Shunt) can be surgically placed to drain cerebrospinal fluid straight from the ventricle. Shunts are known for failing and often need a multitude of revisions, but even with all the revisions, it is less invasive than a decompression. Shunts under the foramen magnum should never be used as a means of controlling ICP.
For the IH/IIH patient, herniated tonsils should be assumed an Acquired Chiari Malformation (even if a small posterior fossa is evident), and by correcting the high pressure before decompression, the decompression will be less likely to fail.
Helpful Tips: If you have IH/IIH, it is best to avoid caffeine, avoid progestin based birth control, and all EDS patients should try to avoid the use of fluoroquinolones such as ciprofloxacin (Cipro), levofloxacin (Levaquin/Quixin), gatifloxacin (Tequin), moxifloxacin (Avelox), ofloxacin (Ocuflox/Floxin/Floxacin), norfloxacin (Noroxin), due to the increased risk of aneurysm.
[wpedon id=”4396″ align=”center”]
References:
1 Rangel-Castillo, Leonardo, et al. “Management of Intracranial Hypertension.” Rangel-Castilla, Leonardo et al. “Management of intracranial hypertension.” Neurologic clinics vol. 26,2 (2008): 521-41, x. doi:10.1016/j.ncl. Feb. 2008, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2452989/>.
2 Aiken, A.H., et al. “Incidence of Cerebellar Tonsillar Ectopia in Idiopathic Intracranial Hypertension: A Mimic of the Chiari I Malformation.” American Journal of Neuroradiology; Nov. 2012, <http://www.ajnr.org/content/33/10/1901>.
3 Mokri, B. “The Monro-Kellie Hypothesis: Applications in CSF Volume Depletion.” Neurology., U.S. National Library of Medicine, 26 June 2001, <https://www.ncbi.nlm.nih.gov/pubmed/11425944>.
5 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 21 Feb. 2017, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
7 Hingwala, Divyata R., et al. “Imaging signs in idiopathic intracranial hypertension: Are these signs seen in secondary intracranial hypertension too?.” Annals of Indian Academy of Neurology vol. 16,2: 229-33. doi:10.4103/0972-2327.112476, June 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3724081/>.
8 Mollan, Susan P., et al. “A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertension.” Practical neurology vol. 14,6: 380-90. doi:10.1136/practneurol-2014-000821. May 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4251443/>.
9 Thurtell, Matthew J., and Michael Wall. “Idiopathic Intracranial Hypertension (Pseudotumor Cerebri): Recognition, Treatment, and Ongoing Management.” Current Treatment Options in Neurology, U.S. National Library of Medicine, Feb. 2013, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3554852/>.
10 Pérez, Mario A., et al. “Primary spontaneous cerebrospinal fluid leaks and idiopathic intracranial hypertension.” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4: 330-7. doi:10.1097/WNO.0b013e318299c292, Dec. 2014, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>.
TETHERED CORD SYNDROME (TCS) INVOLVES A STRETCHING OF THE SPINAL CORD, AND OFTEN YOUR MEDULLA OBLONGATA AS WELL, WHICH LEADS TO A HOST OF NEUROLOGICAL PROBLEMS.
Before we talk about Tethered Cord Syndrome, let’s first talk about the anatomy associated with the spinal column (in layman’s terms).
• The role of the vertebral column is to hold the spine strong (so it can be upright) and protect the spinal cord from injury. In a normal vertebral column, there are thirty-three vertebrae on each side (seven cervical vertebrae, twelve thoracics, five lumbar, five fused vertebrae in the sacrum and another four fused vertebrae in the coccyx).
• Each vertebra in the upper twenty-four vertebrae is separated by intravertebral discs largely composed of the fibrous protein, collagen. The main role of these discs is to allow the vertebral column to move and flex.
• The role of the spinal canal is to hold cerebrospinal fluid around the spinal cord, which not only cushions the cord against injury, but it also lubricates the cord, cleanses the cord, and brings essential nutrients that the spinal cord needs. The spinal canal is made up of several layers that form the meninges. These layers are also composed of high concentrations of collagen. The outermost layer of the meninges is the dura mater. The dura mater should be dense and strong, so cerebrospinal fluid cannot leak from it.
• The spinal cord relays messages from the brain to the nerves that allow the body to function. When part of the spinal cord is compromised, it can inhibit signals from getting to the nerves from that point downward. The brainstem (midbrain, pons, and medulla oblongata) is attached to the spinal cord at the top (the medulla and spinal cord meet at what is called the cervicomedullary junction) and the spinal cord continues down to the mid/lower back. From there it becomes a delicate elastic band of fibrous collagen-based tissue called the filum terminale that extends from the conus medullaris (the lowest point of the spinal cord before it becomes the filum terminale) to the dural sac at the S2 level.1
Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.2 Like Chiari, it is a neurological disorder; however, it is one of the spinal cord.3
Tethered Cord happens when the sticky fibrous tissue of the filum adheres to fatty/scar tissue or the dura lining of the spinal canal.1 While this tethering can happen anywhere in the spinal canal, it is most common at the lumbosacral level.4 When the tethered filum pulls the spinal cord tightly enough that it causes neurological problems, it becomes known as Tethered Cord Syndrome (TCS). Tethered Cord is most common in patients with Spina Bifida (myelomeningocele, meningocele), Spina Bifida Occulta (lipomeningomyelocele, lipomyelocele) and patients with Ehlers-Danlos Syndromes (EDS), a Hereditary Disorder of Connective Tissue (HDCT) where one or more of the types of collagen (the most abundant protein in the human body) is mutated at a cellular level. Tethered cord can be congenital or acquired. It can be obvious in childhood or symptoms may not present themselves until adulthood. Some children may develop minor signs that are overlooked by untrained medical professionals and can progress slowly or rapidly over time.
A Tethered Cord Syndrome diagnosis can be somewhat of a challenge. The signs and symptoms of the condition are not always present and when they are, they are often not recognized, so it is important to know all indicators. People with Tethered Cord (TC) can have sacral dimples, discoloration, and hairy patches on their lower back that can lead a doctor to investigate further, however, some have no external signs at all. Some have kyphosis (rounded back) and scoliosis (curved spine). Sometimes radiological criteria are not met or are ambiguous, yet an Occult Tethered Cord (characterized by the presence of symptoms with normal conus position and inconclusive findings of the filum) can still exist.5 Symptoms can be elusive as well and can happen all at once or gradually over the course of many years. Many symptoms worsen due to activity; climbing stairs has been reported as causing pain that varies from uncomfortable to excruciating.
One of the reasons that Tethered Cord is often overlooked is that many neurosurgeons are not aware of the connection it can have with a Chiari Malformation and the medical tests used for determining if a tethered cord problem exists are not always accurate or accurately read.
Magnetic Resonance Imaging (MRI)
• A lumbar MRI is usually the first step. This gives a visualization of the spinal cord in relation to the surrounding vertebrae. The actual tethering is not always obvious on MRI, sometimes the only proof of the tethering is the pulling it creates on the spinal cord. Doctors will look for the position of the conus medullaris when looking for signs that the spinal cord is being pulled. The consensus amongst most surgeons is that a normal conus should be located from the T12 to the lower L2. There is much debate on the importance of establishing evidence of a low-lying conus.5 When conus reaches the lower L2 or below, doctors should be investigating why it’s low and consider if the cord might be tethered. When looking for the location of the conus, your position can make all the difference. MRIs are generally performed supine (lying down) and the cord is not pulled as tightly as it is when upright. For this reason, upright MRIs are becoming the method of imaging preferred by most neurosurgeons looking to confirm or deny if tethering exists in a patient showing symptoms. Other signs of tethering that might be visible in a lumbar MRI include an enlarged foramen magnum, thick or fatty filum, presence of fatty tissue inside the canal, or the filum might be pulling to one side of the canal.5
• A prone MRI of the lumbar region can be an invaluable tool for those where other MRIs indicate that the filum might be pulling to one side (usually the back side) of the canal. With prone MRIs, imaging is done while the patient is lying face down (as opposed to facing up, like most supine MRIs). If the anteroposterior conus movement of >10% of the canal width was evident from the supine to the prone, then the likelihood of it pulling to one side do to tethering is less likely and more conservative management might be better appropriate than a surgical release.6
• A cervical MRI can also show signs that a tethered cord might exist. The cervical spinal cord can sometimes appear narrow from it being pulled tight. The medulla oblongata can become elongated. This happens because the brainstem is attached to the top of the spinal cord and that cord is being pulled tight, essentially pulling everything down and tight. This elongation of the medulla from the tethering can cause secondary symptoms by itself, known as Dysautonomia.
· Low/herniated cerebellar tonsils consistent with what is seen in a Chiari Malformation. When the brainstem is herniated (where part/most of the medulla is below the foramen magnum) along with the cerebellar tonsils, it is considered a Chiari 1.5 (which should be a good indicator that you might be dealing with an Acquired Chiari Malformation, where the herniated tonsils are secondary to another condition). One study quoted that out of 2,987 patients with a tonsillar herniation of 5mm or greater, 14% met the diagnostic criteria (based on “generally accepted clinical and radiographic criteria”) and 63% of the 289 patients with tonsillar herniations of < 5mm.5
· A syrinx is common with Tethered Cord, as it causes a blockage of fluid at the foramen magnum. A syrinx can develop anywhere in the spine, usually in the lower cord, but with Tethered Cord Syndrome it can develop in the lower medulla (Syringobulbia) as well because of the low brainstem is at the point of the blockage of fluid from the Chiari Malformation.
Even with an upright MRI and every symptom listed, patients are often told they do not have Tethered Cord. This is simply due to a lack of education on the subject and medical bias between doctors. It is important to make sure that you have the images viewed by a neurosurgeon that is familiar not only with Tethered Cord but Chiari and Comorbids as well. (Nearly half of the large study quoted above were referred following a failed Chiari Decompression.5) The combination of the images and the patient’s symptoms should tell the neurosurgeon if surgical intervention is required. Patients often require several consultations before they can find a knowledgeable enough physician.
What We Recommend BEFORE DECOMPRESSION is considered: If you have symptoms of TCS, especially if accompanied by any of the MRI indicators mentioned above, it is both reasonable and prudent to ask your neurosurgeon to investigate further before decompression is considered. A Tethered Cord Release Surgery prior to decompression may relieve the tension that is pulling the brainstem and cerebral tonsils downwards reducing the risk of a failed decompression. There is a chance with small tonsillar herniations that the Tethered Cord Release might allow the cerebellar tonsils to rise enough to the point that cerebrospinal fluid flow is reestablished to where decompression is no longer needed. However, failure to release a tethered cord prior to decompression surgery increases the likelihood of a failed decompression. (In fact, in the study quoted above, out of the 3,276 patients with herniated tonsils, 46% of them were referred for evaluation after a failed decompression surgery.5) An MRI of all three levels of the spine should be done to rule out other possible causes for leg/back symptoms along with urodynamic testing, an Electromyogram (EMG) Test and Nerve Conduction Study (NCS) of the lower limbs is also suggested.
TREATMENT OPTIONS:
For some, physical therapy can help with symptoms for a while. However, ultimately it will likely need to be surgically treated with a Tethered Cord Release.
Tethered Cord Release (TCR) Surgery involves the untethering of the spinal cord. An incision is made in the lumbar area, the filum terminale is separated and the factors that are tethering the spinal cord to the vertebrae are severed. Surgical treatment is not without risk and does not guarantee relief of symptoms. However, in a large study, up to 83% of adult patients report relief, 16% unchanged, and 1% report feeling worse.5 In children, the numbers are even better with 93% obtaining improved symptoms and 7% unchanged.5 Most patients describe the surgery as extremely painful for the first two weeks and “better than they ever remember feeling” (often because they have been tethered for much of their lives) after two weeks. The most common complication involves retethering (often from the scar tissue from the release) and multiple surgeries may be required over a lifetime. Finding a neurosurgeon experienced with TCRs and the surgical treatment of Ehlers-Danlos patients can sometimes help reduce the risks associated with scar tissue formation, but scar tissue can happen with even the best of neurosurgeons.
For the TCS patient, herniated tonsils really should be assumed an Acquired Chiari Malformation (even if a small posterior fossa is evident), and by correcting the tethered cord before decompression the decompression will be less likely to fail.
Special Note: There are other conditions that can present with similar symptoms. Diastasis Recti is a type of abdominal hernia common to pregnant women, those with obesity, and EDS patients. This separation in the abdominal muscles is known to sometimes cause lower back pain and many of the same pelvic floor problems seen with Tethered Cord Syndrome (TCS). Unlike TCS however, it does not usually require surgical treatment. If you suspect Diastasis Recti, we recommend that you talk to your Primary Care Physician about referring you to physical therapy to bring your abdominal muscles back together before considering Tethered Cord Release (TCR).7
[wpedon id=”4396″ align=”center”]
References:
1 Henderson, Fraser C., et al. “Neurological and Spinal Manifestations of the Ehlers–Danlos Syndromes.” American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 21 Feb. 2017, <www.onlinelibrary.wiley.com/doi/10.1002/ajmg.c.31549/full>.
2 “Section of the Filum Terminale Surgery for Tethered Spinal Cord Syndrome in Patients with Chiari Malformation and Syringomyelia.” North Shore-Long Island Jewish Health System The Chiari Institute, Chiari Connection International, 02 Oct. 2006, <http://www.chiariconnectioninternational.com/docs/TCS_SFT_Explained.pdf>.
6 Aoun, Salah G., et al. “The Use of Prone Magnetic Resonance Imaging to Rule Out Tethered Cord in Patients With Structural Spine Anomalies: A Diagnostic Technical Note for Surgical Decision-making.” Cureus vol. 11,3 e4221. 11 Mar. 2019, doi:10.7759/cureus.4221. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6510567/>.
When you start to educate yourself on a condition like Chiari, your vocabulary will be challenged. Most of us study with a medical journal article opened in one tab and medical dictionary in the next. Amongst all the medical terminology you will tackle, there are probably a few terms as important to your understanding of Chiari than comorbidities and pathological/etiological cofactors. When two or more conditions tend to co-occur, they are said to be comorbid with one another. It makes no inferences of a causal relationship between the conditions, only that they co-occur. This co-occurrence deduces that a correlation exists, but when the nature of that correlation is not known, they are just said to be comorbidities. When a “causal relationship” is known or suspected, the conditions start being discussed in terms of pathology or etiology, which are similar, but not exactly the same thing.
An etiological cofactor exists when the “root cause” of a condition is known or believed to be known. That “root cause” is the etiological cofactor. When an etiological cofactor can cause a series of events or conditions that can become “direct causes” for other conditions, that series of events creates a pathology. Conditions along the path are called pathological cofactors. Understanding these cofactors is imperative in understanding Chiari and all of the comorbid conditions that accompany it.
ETIOLOGICAL COFACTOR:
Chiari Malformation often seems like a beast that wreaks havoc on our bodies on every level. Indeed it is, but as you can see from the diagram above, it really is not the “root” of everything that is going wrong. There is a bigger beast at work in so many of us, and its name is Ehlers-Danlos. It is not by chance that so many of us with Chiari have so many other conditions in common (especially conditions like Degenerative Disc Disease, arthritis and other connective tissue problems). It is not by chance that so many of us have a history of miscarriage and similar familial histories. It is not by chance that Chiari is more prevalent in females than males. And it is definitely not by chance that Chiari is running in families and they cannot find a definitive genetic link. They cannot find it because they are not looking at the beast hiding in the background.
Ehlers-Danlos Syndromes are a group of inherited disorders involving a genetic mutation in one or more of our bodies’ collagen. Collagen is the most abundant protein, making up 1/3 of the proteins in the human body, affecting our bones, skin, muscles, and connective tissue[1]. Collagen is often described as a “cellular glue” that helps hold the body together. When that glue fails to hold, everything seems to go awry; before and after birth: skulls can under-develop in utero, organs tend to prolapse, and bones begin to shift as joint laxity increases (including the bones/vertebrae at the craniocervical junction). Ehlers-Danlos is a primary “root cause” of Chiari Malformations and a majority of the other problems we have. The list in blue is far from being a complete list of conditions caused by EDS. They are commonly accompanied with Chiari because they can cause or attribute to a Chiari malformation (pathological cofactors).[2]
PATHOLOGICAL COFACTORS:
Cranial Settling occurs when the skull has dropped and the odontoid (C2/axis) enters into the foramen magnum (Basilar Invagination). This drop can further compromise the craniocervical junction and as it pushes everything down, it increases the likelihood of an Acquired Chiari Malformation.
Craniocervical Instability (CCI) & Atlantoaxial Instability (AAI) usually occurs with cranial settling and Basilar Invagination (BI). The settling and/or softening of tissue can cause a shifting of the C2 (resulting in CCI or AAI) and the cerebellar tonsils (which are already inclined to prolapse) simply drop down with each shift affecting ones ability to tilt/rotate their head.[3]
Intracranial Hypertension (IH – High Intracranial Pressure) occurs when your intracranial pressure (ICP) becomes elevated. This elevation can happen for a variety of reasons.
Space Occupying Masses (cysts, tumors or hydrocephalus) take up space inside the skull causing a “mass effect.”
When no mass effect exists, many doctors look no further and give the diagnosis of Idiopathic Intracranial Hypertension.
Because the area of the skull is fixed in an adult cranium and partially fixed in that of a child, the elements inside the fixed space (CSF, blood volume and brain matter) tend to get pushed out wherever they can (the only place that they can escape without breaking through the dura is through the foramen magnum and the brain matter that’s closest to the foramen magnum is the cerebellar tonsils).[4]
Tethered Cord Syndrome occurs when the tissue inside the epidermis adheres to the spinal cord or filum terminale. While this tethering can happen anywhere along the spinal canal, it is most common in the lower lumbar and/or sacral spine. When this adhesion happens it creates a pulling down of the spinal cord and consequently, the brainstem located at the top of the spinal cord and the cerebellar tonsils just get pulled down with it.[5]
Intracranial Hypotension (Low Intracranial Pressure, often involving a CSF Leak) usually involves a cerebrospinal fluid leak or an over-draining shunt, we will highlight the former. Ehlers-Danlos patients tend to have weak dura matter. Tears/holes in the dura can happen anywhere in the dura surrounding the brain or spinal canal and they can happen completely spontaneously (without a known cause). When the leak occurs in the spinal canal, they can create a suctioning effect where cerebrospinal fluid (CSF) is being pulled down and out, causing the intracranial pressure (ICP) to drop. The cerebellar tonsils that are already prone to prolapse (due to EDS) end up getting suctioned downward with the CSF.[6] Cranial leaks often happen when high pressure is left untreated until the high pressure causes a leak in the dura mater. In cranial leaks, fluid usually leaks through the nose or ears (less common), and you can often taste the metallic taste of the cerebrospinal fluid in the back of your throat. While both spinal leaks and cranial leaks can cause low pressure and low-pressure symptoms, and while both can start, stop, and start again spontaneously, there is an increased risk whenever there is an opening where cerebrospinal fluid leaks outside of the human body (if cerebrospinal fluid can make it out of the body, microscopic bacteria can make it inside the same opening where it can enter in the meninges).[7]
Posterior Cranial Fossa Hypoplasia (PCFH) is the only etiological cofactor listed above that is definitely congenital. The role of collagen in bone development has been long-standing, especially its known contribution to certain conditions like Osteogenesis Imperfecta. However, more recent studies are discovering the role collagen plays in congenital posterior fossa anomalies. Posterior Cranial Fossa Hypoplasia is the most commonly “acclaimed” cause of Chiari malformations, but studies show, that even when all of the other causes above are factored out, only approximately 52% of those left (that fail to meet “the diagnosis criteria” for any of the above), have a small posterior fossa.[8]
COMORBIDITIES:
While all of the conditions listed in the diagram are comorbidities, some are etiological/pathological of an Acquired Chiari (even though nearly 100% of us are told that our Chiari Malformation is congenital) and others have Chiari Malformation as their etiological/pathological cofactor:
Syringomyelia occurs when cerebrospinal fluid (CSF) is obstructed and a CSF filled cyst/cavity forms inside the spinal cord. This cyst is directly related to the obstruction of cerebrospinal fluid that can be caused by Chiari Malformation, Spinal Stenosis (a narrowing of the spinal canal, spinal cyst/tumor, a herniated disc), or irregular curvature of the spine (scoliosis). When that cyst/cavity extends into the medulla oblongata (the lowest part of the brainstem), it is called Syringobulbia, and it comes with a new set of symptoms consistent with the damage being done to the brainstem. So when Chiari Malformation exists with a syrinx, and there is no stenosis or disc problem in close proximity below it, the Chiari Malformation should be listed as the etiological condition of the syrinx. If more than just the Chiari Malformation is believed to be causing the syrinx, each would be more accurately described as pathological.
Dysautonomia occurs when damage has been done to the brainstem or Vagus nerve. Whenever either of these is damaged, often from compression at/near the craniocervical junction, the autonomic nervous system can begin to dysfunction.
Confused? If you understand the causal relationships but find yourself wondering if a comorbid condition is an etiological or a pathological, think of it in terms of a domino effect. Only the first domino is etiological. All of the dominoes in between (on the path) are pathological. The important thing to remember in this array of medical terminology is that while everything is definitely not Chiari, it almost always shares a connection to it, and that is why so many of us have so many conditions and symptoms that doctors call unrelated! It is imperative in our fight that we know “what” we have and “why” it is happening. With such a broad spectrum of symptoms (like we all have), we must educate ourselves and not just believe the limited knowledge of our doctors.
7 Pérez, Mario A et al. “Primary Spontaneous Cerebrospinal Fluid Leaks and Idiopathic Intracranial Hypertension” Journal of neuro-ophthalmology : the official journal of the North American Neuro-Ophthalmology Society vol. 33,4 (2013): 330-7. doi:10.1097/WNO.0b013e318299c292, <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4040082/>
“Vi måste operera din hjärna och det måste ske nu”!
Vad gör du egentligen om någon säger så till dig? Hjärnan. Den där delen högst uppe som liksom är allt som du är. Någon måste skära i den och fixa något som är fel. Och att det finns ingen tid att tänka efter. Hur ska du kunna stanna nu och säga: Men vänta lite, det finns saker som inte går ihop och jag behöver få svar. Jag hoppas att när du har läst detta så är det just precis vad du gör, och du gör det med en stark röst för om du läser detta så är chansen stor att även du är en krigare och för denna fighten så kommer det behövas.
Våren 2017 var jag den lyckligaste människan på jorden. Vi skulle äntligen bli en liten familj. Vi hade längtat och planerat i flera år för en liten människa och till slut kröp pluset fram på stickan. Jag trodde inte jag kunde vara lyckligare än då. Tiden gick och vi levde i vår lyckobubbla. Jag var van vid att få ont i huvudet när jag skrattade, hostade eller nös och trodde att detta var något som hände alla – men helt plötsligt började jag få riktigt ont i huvudet. Läkaren på vårdcentralen sa att det hörde till graviditeten och jag skulle inte oroa mig. Jag försökte ignorera symptomen men de eskalerade snabbt med dålig balans, jag tappade styrka och koordination i armar och ben, såg dubbelt och hade stora svårigheter med minne och koncentration. Till slut gick jag till läkaren igen som nog ändå tyckte att jag skulle till akuten för och magnetröntgas. Jag kunde ju ha fått en hjärnblödning.
Efter röntgen satt vi där jag och min sambo i vårt lilla rum på akuten och skrattade och skojade som vi alltid gör. Sambons ADHD gjorde att han klättrade på väggarna och roade mig för att jag skulle slippa tänka på smärtan. Tanken slog mig: “Vi kommer bli världens lyckligaste familj, han och jag och våran lilla bebis.” En AT-läkare kom in, tittade konstigt på mig och frågade hur jag mådde. Jag svarade att jag gjorde mitt bästa trots att det var jobbigt. Han började göra några tester, sa ingenting men kollade sen på mig igen och sa: “Du har en missbildning i hjärnan. Det är därför du mår som du gör”. Han förklarade att min lillhjärna låg i kläm och att jag inte fick åka hem förrän han pratat med specialister på ett annat sjukhus. Så de la in mig. Jag visste ingenting om resan som nu började, inte ens vad det var jag hade. När jag låg i sjukhussängen så försökte jag googla mig fram till svar och undrade mest vad framtiden skulle föra med sig.
Dagen efter kom överläkaren in till mig. Han berättade att min lillhjärna buktade ut 13mm från skallbasen och att de helst av allt velat skicka mig på operation på en gång eftersom jag hade så svåra besvär, men med tanke på lilla bebisen så fick det lov och vänta tills den var säkert ute. Utanför mitt fönster började världen göra sig redo för sommaren och i kalendern stod det Juni 2017.
”Arnold Chiari” (Chiari typ 1). Så sa de att det hette och google förklarade för mig varför jag hade mått som jag gjort. Allt stämde ju in och armerad med kunskap så kändes det ändå lite tryggare att komma hem medans vi väntade ut bebisen. När jag surfade runt på nätet så hittade jag en grupp på Facebook som var för just sådana som mig och jag hade plötsligt några att bolla detta med. Några som gjort samma resa som jag skulle göra. Man kan säga att jag höll mig uppe den där tiden hemma med tankarna på att jag gjorde det för någon annans skull. För vår lilla familjs skull. Så när jag i vecka 20 kom in på ett ultraljud var jag inte alls beredd på vad som hände. Vårt barn hade inte utvecklats som det skulle och den enda utvägen var att låta kroppen stöta bort vår dröm. Jag föll rakt ned i ett mörkt hål och jag minns faktiskt inte alls så mycket av den tiden. Det var för mycket att hantera sorgen av både min egen sjukdom och att vårt barn aldrig fick bli. Världen kändes grym och jävlig.
I oktober fick jag träffa min första neurokirurg och vi fick direkt veta att det var ett allvarligt fynd och att jag borde opereras så fort som möjligt. När jag satt där så försökte jag komma ihåg alla tips på frågor jag fått från min grupp på Facebook, att jag skulle fråga om retroflexed odontoid, bindvävsstörningar och instabila nackar. Men ingenting kändes som om det hade fastnat fast jag hade studerat på alla dessa komorbiteter och jag hade inga argument när läkaren sa att det var en operation som gällde. Det var inte det att jag inte trodde att de där sakerna gällde mig, tvärtom hade jag flera symptom på EDS men neurokirurgen sa att om jag hade haft en bindvävsstörning så hade de märkt av det innan och att jag behövde en dekompression och duraplastik just i detta läge. I efterhand så kan jag se att detta var ett avgörande ögonblick och jag önskar att jag kunde gå tillbaka och ändra historien. Så du som läser detta nu, lyssna noga. Jag vill att du bestämmer dig för att kräva att din läkare utesluter alla eventualiteter som kan orsaka en lillhjärna att ektopera för det är inte alla som har Chiari som är födda med en för liten posterior fossa, som många kirurger kommer vilja få dig att tro. Jag vet att det kan kännas svårt och sitta där mitt emot någon som ska ha all kunskap och att du vill kunna lita på att det de säger är rätt och riktigt, men komplikationerna av en sådan operation OM du faktiskt har chiari av någon annan anledning är inte värda det. Tro mig, eller för all del – fortsätt läsa så ska jag förklara.
I mars 2018 tog läkarna bort 2,5 cm skallben och 2cm på min atlaskota. När jag vaknade så mådde jag bra, förutom att de glömt stänga mitt ena öga innan de la mig nedåt på britsen så det gick sönder (Yes, sånt händer). Det tog ett tag innan det läkte och jag har idag ärr på hornhinnan som aldrig försvinner. Trots ögat så kände jag mig ändå okej, men det hela varade bara i två veckor innan jag fick en kemisk hjärnhinneinflammation och fick ligga inlagd på sjukhus igen. Väl hemma så väntade och väntade jag på att få må bättre, men det hände helt enkelt inte. Huvudvärken var fortfarande jobbig, jag kunde inte ligga på rygg eller bakhuvudet utan att känna som om jag skulle svimma, jag var svag, yr och en hel del neurologiska besvär i form av känselbortfall och smärta. Läkarna försökte alla möjliga mediciner, men allt gav mig biverkningar och ingenting fungerade egentligen. Jag fick välja mellan bisarra svåra biverkningar och att stå på morfin och som du kanske vet så är inte läkare alldeles för förtjusta i opiater mot långvarig smärta. Hur mycket läkarna än försökte justera medicinerna så var det ingenting som jag kunde ta. Jag hade ont.
”Det måste gå ett år för att du ska kunna läka innan vi kan ta några beslut om din hälsa”. Jag fick höra detta flera gånger när jag försökte prata med läkarna om hur jag mådde. ”Du är beroende av morfin”, ”Du är narkoman”, ”Din smärta är inte på riktigt, du bara inbillar dig”, ”Du är botad nu och ska inte ha så här ont, din hjärna hittar på”. Detta är saker jag fick höra gång på gång. Efter en träff med min neurokirurg så fick jag en röntgen med flexion och extension för att kunna se över RO, CCI och EDS och fick snabbt veta att ingenting var fel på bilderna. Jag mådde bra enligt alla bilder. EDS-utredning skulle ta tid och det ville inte läkarna göra förrän efter mitt ”läknings år” gått. Vad jag än frågade läkarna om så fick jag samma svar. Det är inget fel på dig eller du måste läka klart. Men min kropp ville inte läka och jag skrev flera meddelanden till min kirurg utan att få svar.
”Hjälp mig, det känns som om jag ska dö”, i december 2018 skrev jag ett långt meddelande med alla symptom, hur ont jag hade och att jag trodde att min kropp höll på att ge upp och det tog inte lång tid innan han faktiskt ringde upp och vi pratade länge. Det fanns inga anledningar till att jag skulle må såhär dåligt, det enda bilderna hade visat var ett litet bråck som inte skulle påverka och en inkapslad vätskecysta. Han kände sig rådvill och sa att han skulle ta upp mitt fall med några andra kollegor och kirurger på en konferens för och se om någon annan hade någon tanke. Igen påpekade han att jag inte kunde vänta mig någon åtgärd innan mitt läkningsår var över och jag kände mig frustrerad. Jag va botad sa dom, men ändå kändes det som att jag höll på att dö succesivt.
Min främsta fiende var nu tiden och den sniglade sig fram. Snart var det februari 2019. 11 månader efter att jag fått min första operation. Jag kunde inte längre klara av en vardag, jag sov mestadels under dagarna och jag hade så väldigt ont. Min sambo tog hand om hemmet och mig. När jag låg på rygg så svimmade jag och livet var outhärdligt. Jag skrev återigen ett meddelande till min kirurg och denna gång tog jag helt enkelt farväl. Jag kände hur livet rann ur mig och det fanns snart inte mer tid kvar. Han ringde upp nästan på en gång och berättade att de nu tänkte göra en till operation. De hade fortfarande inga indikationer och ville göra några tester innan jag fick operationstid. Jag fick göra neurologiska tester, en magnetröntgen och en lumbalpunktion för att kolla trycket i skallen. Magnetröntgen fick jag göra under narkos eftersom att jag inte kunde ligga på bakhuvudet och tryckmätningen visade att mitt tryck låg lite högt. Neurologen tyckte att jag var tjock med ett par kilo extra för min längd så de la inte någon vikt vid resultaten men efter testerna så fick jag tid för operation igen. April 2019.
”Hade jag sett dessa bilder på någon annan patient så hade jag inte gjort någonting. Egentligen finns det inget problem”. Det berättade neurokirurgen för mig när jag skrevs in medans han också berättade vad de skulle göra. Gå in, ta bort bråcket, utöka duraplastiken och sätta en titanplatta för att framhäva kompressions-effekten som kom sig av att jag låg på rygg. Han hade kunnat säga vad som helst så länge de gjorde operationen och jag mådde bättre, för mitt liv var inget liv – det var ett väntrum till döden. Och det visade sig att det var just och precis det.
”Petra, detta är bland det värsta jag har sett” – orden kom ur hans mun när han träffade mig på uppvaket och han fortsatte och berätta att jag hade haft massiv ärrvävnad som de inte kunnat se på röntgen, den värsta han sett i hela sin karriär. Hade de väntat längre med en operation så hade jag blivit hjärndöd. När de öppnade skallen så hade jag ingen pulsfrekvens i hjärnan och inget flöde alls på csv vätskan. Ärrvävnaden och bråcket hade satt stopp för allt, och som om det inte var nog så hade allt också vuxit fast i varandra. Hinnor, lillhjärna och ryggmärg hade blivit som en enda stor smet.
Nu var jag återigen botad och skulle åka hem, även om jag redan på sjukhuset fick starka smärtgenombrott som var nästan omöjliga att hantera så tyckte läkarna att jag nu var fixad och skulle vara hemma. Jag önskar att jag kunde säga att läget har blivit bättre. Att läkarna nu lyssnar på mig och förstår att ärrvävnaden kan växa tillbaka men så är inte fallet med alla. En del tycker att jag är nu botad och ska må bra. Idag är det 6 månader sedan jag opererades och jag börjar nu vara i samma situation som för ett år sedan. Jag har väldigt ont, börjar tappa neurologiska funktioner och min vardag finns inte. Mina ”måsten” består numera av ”Jag måste lindra smärtan” – inget annat får rum på min planering.
För ett tag sedan ringde min kirurg och frågade hur jag mådde. När jag berättade hur jag hade det så sa han att de nu inte vågar göra något mer kirurgiskt. Jag tog då återigen upp frågan om EDS och sa att det nu var dags att utreda det eftersom att jag har så många symptom som tyder på knasig bindväv. Du kanske tror nu att han genast förstod vad jag pratade om och var med på noterna? Nej. Hans svar var: Du har väl inga andra besvär än din Chiari? ”Va? Nu räcker det! I två år har jag pratat om en utredning för att ta reda på vad som egentligen är fel på min kropp, har du inte lyssnat på mig ett dugg” Det tog stopp. Det fick räcka med okunskap och ignorans och jag väntar nu på en utredning för bindvävsstörning.
I dagsläget när jag skriver detta så vet man inte någonting egentligen gällande mig. Varför allt är som det är och varför jag blir så sjuk. Jag är ett stort frågetecken hos sjukvården, så jag gör vad vi måste göra i denna situation. Jag läser på, pluggar och kämpar. Vågar fråga och är jobbig. Jag tar hjälp av personer som går i samma skor som jag och utan communityn på Facebook så vet jag inte vad jag hade gjort. Jag svarar på frågor jag inte borde behöva svara på när jag kommer till vårdcentral eller sjukhus ”Vad sa du att du hade sa du?” , men jag hade inte orkat kämpa om jag inte haft känslan av att jag inte är själv. Jag tror inte att någonting kan hända mig nu som jag inte redan gått igenom, men skillnaden nu är att jag har mer kunskap och erfarenhet men jag är också utmattad, trött och stundtals nedslagen av att behöva slåss. Att gå igenom så pass stora och allvarliga operationer utan att bli frisk är inte helt lätt att hantera alla dagar. Man ska ju liksom inte bli lika dålig, om inte sämre – efteråt. Man ska ju bli botad.
Nu när du har läst ända hit så vet jag att du förstår att det är så viktigt att du krigar redan från början. Oavsett om de säger att du måste opereras nu nu nu – KRÄV svar. Se till att alla diagnoser som kan vara av vikt är utredda. Har du en läcka i ryggen, i kraniet, kanske har du bindvävsproblem eller för högt tryck i huvudet. Kanske är det någon anledning till att din lillhjärna håller på och trycka sig ut ur det där hålet och kanske är inte den anledningen att du är född sådan. Ta råd av de som vet och lär dig. Jag vet att det är jobbigt, jag vet att du inte vill och jag vet att det finns dagar då du bara vill lägga dig ned och gråta och slippa vara stark. Så – gör det då – det är okej, men sen ställer du dig upp igen och fortsätter kriga.
Tiden är inte alltid vår vän, oavsett om det gäller väntetid på hjälp, väntetid på operation och recept eller bara den tid du får utstå dumma frågor och människor som egentligen ska hjälpa dig som misstror dig. Tiden du måste lyssna på någon som tror att du inbillar dig eller tiden det tar innan du hittar en läkare som lyssnar och tror på dig och när du väl har den läkaren och hen lovar dig att allt kommer blir bra så är det lätt att säga “Ja” utan att tänka, men det är då tiden är som viktigast. Det är då du ska vänta INNAN någon har för alltid förändrat hur din skalle ser ut och kanske skapat värre problem än du hade innan. Så ta din tid och se till att du har alla svar innan så att du kan spendera din tid med att läka och leva ditt liv igen efteråt.
“We need to perform surgery on your brain, and we need to do it now!”
What would you do if someone said that to you? Your brain – that thing on the top of your head that is all that is you. Someone needs to cut into it and fix what is wrong and there is no time to think. How are you supposed to say, ”Stop, I need to think. There are questions without answers and I need answers.” Well, I do hope that once you have read this – that is exactly what you will do and you will do it with confidence and a strong voice. Why? Because if you are reading this, chances are you are a warrior too, and to fight this fight successfully, you will need to see yourself as a POWERFUL WARRIOR!
It was spring 2017 and I was the happiest gal in the world. We had planned and longed for years and we were finally becoming a family. I could not have been happier. At that time, I was used to getting headaches when I coughed or sneezed, but I figured this happened to everyone. I would never have thought that something was wrong, but all of a sudden I started getting real headaches and I went to the doctor’s office. They said that it was just the pregnancy and that I didn’t need to worry so I went on with my life. However, the symptoms were escalating fast and I was losing my balance, strength, and coordination, and I had major issues with remembering and focusing. When I finally went to the doctor again, they sent me straight to the ER to get an MRI to rule out a stroke.
As we sat there in that tiny room, we were laughing and giggling. My boyfriend tried to keep my spirits up and with ADHD, he was pretty much bouncing off the walls. I looked at us and thought ” We will be the happier family. Him, me and our little baby.” An intern doctor came in through the door and gave me a weird look. ”How are you doing?” he said. I said I was doing my best to not think about the pain. He started doing some tests, but he didn’t really say much. When he was done, he looked at me again and said ”You have a malformation in your brain. That is what is causing your pain and symptoms.” He explained that my cerebellum was pinched and that I couldn’t go home until he had conferred with specialists at another hospital, and then he admitted me. I had no clue about the journey I was about to take and I honestly didn’t even understand what it was I had. I tried Googling that night and I was wondering what the future would hold in store for us.
The next day the head of the department came to see me and told me that my cerebellum was protruding 13 mm from my skull and that they would have wanted me to have an operation immediately, but because of the baby – they would have to wait. Outside my hospital window, the world was getting ready for summer and the calendars now read, ”June 2017.”
They told me I had something called ”Arnold Chiari” (Chiari Malformation Type 1) and Google explained to me why I had been feeling the way I did. Everything fit and I felt a bit safer going home, armed with the knowledge that I could be helped. Browsing Facebook, I found a group of likeminded people and my world suddenly expanded and I felt like I belonged. But the one thing that kept me going was the thought that I was doing this for someone. Not me, but for our tiny family. I had no idea what was coming. One day I was going in for a scheduled ultrasound in our second trimester and the next I was no longer going to be a mom. The doctors told us that our baby wasn’t developing as it should and that they had to let my body reject it. I fell into a deep depression and I honestly can’t remember much of what happened during that time. Dealing with the loss of our dream and my own illness was too much to bear, and I just shut down. The world was a cruel and harsh place.
It was October when I got to meet my first neurosurgeon and I was told that what they had found was considered an important finding. They really wanted me to get on that table as soon as possible. Sitting in front of this highly ranked doctor, I tried to remember all the things that I was supposed to ask. Things I had learned in the group and on Facebook. The retroflexed odontoid, connective tissue disorder connections and unstable necks. But my mind felt like a non-stick surface and I couldn’t remember any of it. It wasn’t that I didn’t think it applied to me – actually the opposite. But every possible idea that I shared with my new neurosurgeon fell on deaf ears, as he would sternly tell me, ”all you have is Chiari and surgery is going to fix that.” I felt intimidated and was afraid to rock the boat. If I had a connective tissue disorder, they would have known, right? I needn’t worry about knowing this, I just needed a duraplasty and decompression and all would be fine. In hindsight, this turned out to be a pivotal point in my fight (and I hope those reading pay particular attention to this point). This is the point where I should have stopped and stood up for myself. Nobody knows our bodies better than we do, we know when something is wrong. I should have listened to my body and trusted my gut. I should have not agreed to brain surgery without additional testing to rule out the possibility of comorbids pathological to Chiari, and not just assume that the only cause of my tonsillar descent was an underdeveloped posterior fossa. Many surgeons say this and are unwilling to test us for any other pathologies before they alter our cranial anatomy. As patients, we believe our surgeons, even when we know that they are simply unwilling to test any further. They believe what is in their textbooks and I am here to tell you that sometimes, they’re wrong and their assumptions are just not correct. I know we want to believe them, but the complications that can arise if we’re right and they’re wrong are not worth it in the end. Believe me, and if you don’t, please just keep reading.
They removed 2.5 cm of my skull bone and 2 cm of the lamina from my atlas vertebra (C1) in March 2018. For two weeks I was fine until I developed chemical meningitis and was hospitalized. Well, fine is maybe an overstatement since they did forget to close my eye before the operation and it actually dried up and stuck to the operating table, scarring my cornea for life (yes, that is a thing). I waited and waited for that moment when I was supposed to feel good again. But it never came. I couldn’t lay down on my back or the back of my head without feeling like I was going to faint, my head pain was awful and I had several neurological symptoms. The doctors tried different medicines and painkillers but nothing worked or it gave me bizarre side effects. No matter what they tried, the pain wouldn’t subside.
”In Sweden, you have to be a year post-operative before we can make any kind of decisions on your health.” This is something I was told so many times and it was so frustrating. I was told that I was an addict to opioids and that I was imagining my pain. ”It isn’t real, you just think it is going to hurt.” Or, ”You are cured and there is no reason you should be in all this pain.” I was fed so many misconceptions and lies during this period, but I had to keep fighting in hopes of getting my life back. Giving up was not an option. After having new MRIs done to look at my retroflexed odontoid and the possibility of instability, I was told I was fine. The pictures were perfect and I wasn’t sick. I was told that an investigation to look into Ehlers-Danlos would take to long and my doctors didn’t think it was important to do before my year was up. They considered me ”well” and I felt worse than ever. If I was cured, why did I feel like I was dying?
In December I wrote to my doctor ”Please help me, I feel like I am about to die.” That must have triggered something in him because he called me on the phone and we talked for a long time. He told me there were no reasons he could see to explain my symptoms. I had a small herniated disc and an arachnoid cyst. Nothing that would cause my pain and symptoms. Even so – he said he would check with some colleagues to see if there was something that could be done, but he was adamant about not touching my brain until I was a year out from my first surgery.
Time was my worst enemy. I couldn’t believe how slowly it went by. February 2019 came and it was 11 months after I first lay on that table. I couldn’t manage the day to day life, I slept all through the day and I was in grave pain. If I tried laying on my back, I would pass out. My boyfriend took care of our house and me, and life was not a life worth living. Once again I tried contacting my doctor. This time I simply wrote a goodbye letter, I knew I was dying. He called me right away and told me that they were going to open me up again. There were still no indications in the images that something was wrong so they asked me to perform some tests before they would schedule me. I did neurological tests, a lumbar puncture, and a new MRI. I had to be put to sleep during the MRI because of my issues and the tests did show my pressure was a bit too high. However, the neurologist thought I had a couple of extra kilos for my height and attributed everything to me being slightly overweight. My second surgery was scheduled in April 2019.
”Had I seen these images on someone else, I wouldn’t have done anything. There is really no visible problem.” My doctor told me this when I was admitted for my surgery. He told me they would remove the herniated disc and the arachnoid cyst, extend the duraplasty and transfer a titanium plate to combat the decompression effect I had of lying on my back. I didn’t really care what he told me they would do – I would have let them put horns on my skull if he thought it would’ve helped. My life wasn’t a life – it was a passage to death’s door, and I didn’t even know how right I was.
”Petra, this is the worst case I have ever seen” – the words out of his mouth when he saw me in the ICU after surgery shocked me. He continued to tell me that I had massive scar tissue that wasn’t visible in the images and that it was the worst case he had seen in his entire career. Had they waited to perform the surgery, I would have become brain dead. I had no pulse frequency in my brain at all and my CSF did not flow. The scar tissue and the herniated disc were now blocking cerebrospinal fluid and it had all grown together like a giant lump of bad juju. Membranes, cerebellum and the spinal canal were like a big jumble.
I was once again cured and sent off to go home and heal. Despite having major issues with pain control that could not even be managed in the hospital, they figured I was fixed and ready to go. I wish I could tell you that it has gotten better, that the doctors finally started listening to me and realized that scar tissue can go back, but they still don’t. Most of them feel like I am now cured and should be fine. I am 6 months out and am starting to feel the same way I felt before surgery last time. I’m in immense pain, losing neurological functions and my day to day life is nonexistent. My pain management is all that is on my schedule and I am functioning on a day-to-day basis. My neurosurgeon called to check up on me a while ago and when I told him how I was doing he said that they didn’t dare to perform any more surgeries on me now. So I asked him about my thoughts on a connective tissue disorder. I was ready for him to give the go-ahead for an investigation. But to my surprise, he said, ”But you don’t have any more issues than your Chiari, do you?” I was done. For two year I had tried to convey what I thought was going on and told him about me and he hadn’t heard or registered a word of what I said. Enough was enough, and I told him that he needed to listen to me and start helping me feel better and find out what was wrong. I am now waiting to look further into my connective tissues and Ehlers-Danlos Syndrome (EDS).
Nobody really knows what is wrong with me and how to handle it. I am a great enigma with my doctors and I can not trust anyone to be my advocate and do the research, so I do it myself. I’ve learned to ask tough questions and not give up and I have also learned to ask for help from people in my position. What are they doing and how can I apply that to my life. Without the community, I would be lost. I would not know what to do when I get to yet another doctor or nurse who asks, ”You have WHAT?” I don’t think I would have had the strength to keep on fighting if I didn’t know that I wasn’t alone. I am pretty sure nothing else can happen now that I haven’t already been through. I have more knowledge and experience, but I am also more worn out, exhausted and sometimes just jaded from having to constantly fight. To go through two major surgeries without any relief is not easy peasy. Sometimes it just sucks – I am supposed to get better from treatments, not worse. Right?
So, I commend you for reading through to this point and hope that by doing so, you now know how important it is for you to suit up for battle. You need to be the warrior from the get-go. No matter if they tell you it needs to get done yesterday – you make sure you have your answers before you agree. Get every answer from your list: Could it be from a spinal leak? A cranial leak? Do I have a connective tissue problem? Could my pressure be causing it? Could it be something else than a congenital malformation that is causing your brain to escape your skull? Study and learn all you can, ask for help and be the pain in the *ss patient if you need to be. I know you don’t want to. I know it is rough and that some days you just wanna lay down and give up. So do that – for a day – and then stand up and fight again! We wait for a lot of things. We wait for urgent care. We wait for prescriptions. We wait for testing. We wait for imaging. We wait for a doctor who will believe us and when one finally does and promises some relief with surgery, we figure we’re done waiting. But THAT IS THE TIME TO WAIT and get all the data before you’re on the other side of surgery, where your anatomy has forever changed and they are telling you that you are healed. I know you think that you are pressed for time, but take time and make sure you have all your ducks in a row and do your very best to make sure that nothing is missed, so you can spend time healing and living life again!
When I first started getting hit with symptoms, I was a divorced, single mother of three amazing kids; responsible not only to provide for them but to see them through life, unscathed by life’s situations, and showing them that there was nothing that if they worked hard at something, nothing could hold them back. I had just started to expand in my career as a self-taught auto technician. I was a woman making a place for herself in an industry traditionally dominated by males. July 3, 2015, was the day that my life forever changed. I was brought to the hospital with stroke-like symptoms. I was having visual problems. I couldn’t walk or talk. I had no idea who I was or where I was. The whole right side of my body basically stopped working and the right side of my face was droopy. I was brought to the ER and before the doctor would even try to figure out what was wrong with me, he ordered a series of drug tests. I passed every test, so he finally admitted to me. Once on the neurology floor, more testing was done. They performed an MRI, MRA, EKG and told us that all results were normal. I later discovered that was not the case.
One doctor refused to believe that I was not on drugs. She noted in my file that while she has no evidence to support it, she believed that I am on a drug that they hadn’t screened for, based solely on “my age, single mom status, and prior good health.” She also noted that they found a Chiari, but that based on my symptoms, she believed it was irrelevant (an incidental finding). I would love to see her now and show her just how very wrong she was. I firmly believe that what she put in my medical chart is why I have had such a difficult time getting the care that I need and deserve.
A few days later, I followed up with my PCP. She went over my MRI results with me and pointed out that they found a Chiari Malformation with a 19mm herniation of my cerebellar tonsils. She told me of changes in my white matter that the radiologist said needed to be “further evaluated” and referred me to my first neurologist, who I met within August. He ordered a visual evoked potential and an EEG. Both come back normal, so he diagnosed me with migraines, even after hearing my symptoms, which frustrates me even more as I know that it is not migraines causing these issues.
At this point, I switched my neurology care to another hospital. They went over my history with me and ordered a lumbar puncture to rule out Multiple Sclerosis, which showed banding in my spinal fluid. On September 14, 2015, I was officially diagnosed with Multiple Sclerosis and opted to begin treatment and was to start on Plegridy. As I started the full doses I started breaking out into hives. The docs didn’t seem to think I should worry, so I called the drug manufacturer and they said it should be considered an allergic reaction to the Plegridy, and to discontinue using it and advise my doctor.
After this experience, I switched care back to the first hospital for neurology to get a second opinion. The new neurologist ordered a new brain MRI and one of my cervical spine. There were no changes to my brain MRI, but my cervical imaging showed a syrinx. They weren’t sure if the syrinx was of any significance. So, she referred me to the only MS specialist in North Dakota whom I would meet with, in May. The MS specialist took a complete history on me and ran a bunch of blood work to rule out other illnesses. When those illnesses were all ruled out, she diagnosed me with Radiologic Isolated Syndrome (which means that they saw similar characteristics to MS in my imaging, without MS symptoms). While in her care I continued to get worse, with symptoms progressed to include pins and needles feeling in my hands and feet, occipital headaches that drop me to the ground, cognitive decline, fatigue, weakness, some random numbness, and muscle spasms. She ordered a new MRI and once again no changes were indicated. She began to question if my Chiari was behind my growing number of symptoms. She tried to refer me to Mayo, but my insurance declined her referral.
Eventually, I started having issues walking and my gait was becoming increasingly unsteady, so I return to a local neurology clinic. They did an MRI on my brain, cervical and thoracic spine. They found a syrinx in my thoracic spine and once again they doubted the significance, along with a slight scoliosis convex. When asked what a syrinx was, they told me that it was “an old MS lesion.” I later learned that a syrinx is a cyst inside of the spinal cord caused by a blockage of cerebrospinal fluid and it damages the spinal cord from the inside out – often associated with Chiari Malformation.
During this care for MS, I kept having what they thought were MS relapses, roughly every three to four months. Each time they ordered new MRI images and treated me with high doses of IV steroids for five days in a row. Never once did this imaging ever show an actual MS-relapse or MS activity. I continually had issues with every medication that they put me on to help “try to delay the progression of the MS” (the MS that I never had). In November 2017 I started Ocrevus, which was just FDA approved that year. Around this time, I started having strange symptoms and thought them just to be side effects of the medication, not realizing that something else might be causing it all. I met with my neurologist before my second full dose and I told her everything that I was experiencing. We opted to take me off the Ocrevus and they repeated the MRI yet again. Again, the MRIs show absolutely nothing new for activity and she admits that she doesn’t know what to do for me. I am three years in at that point and never once have they seen any MS activity.
I made an appointment with yet another neurologist. I met with him on March 2019 and he immediately pulled my MS diagnosis. He instead decides that I have migraines and anxiety. He believes that anxiety is why I am completely numb all over my body. He disregards the Chiari and the syrinxes when asked about them stating that they do not cause any symptoms that aren’t of any significance. I left this appointment more frustrated than I was before and began losing hope that I was ever going to be able to figure out what was going on with me. How am I ever going to get the proper treatment when I am consistently blown off whenever I ask about a condition that was noted from day one?
I began working more closely with my PCP. I went over the last three years of my medical journey with her and told her that I felt that we really needed to dig into this Chiari Malformation that has been called out in my imaging since July of 2015, especially since I had many symptoms that may be from it. I told her about a neurosurgeon that I had been told about in Sioux Falls, SD, who specializes in Chiari. We also talk about a connective tissue disorder known as Ehlers-Danlos Syndrome and start comparing my symptoms (of which I had several). My PCP sends in referrals to the neurosurgeon, a genetic counselor, and a rheumatologist. (Because with Chiari you will more than likely have several comorbidities.)
In June we traveled down to the specialist. He went over my MRI images and stated that my herniation was 19mm (which was almost quadruple the amount that they get concerned about). That coupled with my symptoms led to discussing the need for me to have decompression surgery. Finally, after four years we know the true culprit of what was wrong with me, my brain is literally falling out of my skull. We leave with a bunch of literature for the surgery and I call his office back Friday and tell them my decision to go forward with the surgery and we started planning for me to have surgery in early September. Just as we thought everything was on the right course, my insurance drops a bombshell on me. I received a call from the specialist office, and they tell me that my insurance has declined my surgery stating that I can have it done locally by the same incompetent neurosurgeon that I met who couldn’t even measure my Chiari correctly. I have appealed this decision twice and both times I was denied. I am now pushing for a State Fair Hearing.
The last four years have been one hell of a ride when it comes to my health. My health problems have made it far more difficult to continue working on cars. As my symptoms wage war on my body, I am now forced to work on light duty and have been for the last two and a half years. I know that my days of working in a shop are coming to end as I just can’t handle the physical requirements of the job anymore. My quality of life in the last year alone has declined sharply. I used to be the energetic mom who could coach a sports team after working all day in the shop and still have the energy to keep up with the housework, now that is not the case. I manage to push on and get them to their activities, but I’m exhausted to the core. When this all began back in 2015 my kids were 8, 7, and 5. They are now 12, 11 and 9. At times I feel like I am a horrible mother because I miss the mom that I used to be. I miss the days when my kids weren’t worried about my health and when we could make plans with other families and keep them. I have lost so much of who I am thanks to the ignorance of some members of the medical community. I am losing faith in the medical profession in general. Male doctors have been the worst as I go through this journey, as women seem to have to first prove that it’s not psychosomatic before we’re worthy of being helped, even with imaging shows something to the contrary. When I present them with proven facts about Chiari Malformation, it still gets dismissed and it is extremely frustrating. The longer I go without receiving proper treatment, the more likely it becomes that some of this damage will become permanent and to me, that is not acceptable. I am fighting for my life and I will not back down until I receive the proper care, I can’t!










 “But you look so good” is what people usually say when they find out that I struggle with debilitating chronic illnesses. It is true- I wear fashionable clothes, I do my hair, I put on makeup and I have a smile on my face. Underneath it all though, is someone who is trying to live her best life with the cards she was dealt with. I grew up in southern India and none of my family members knew what Chiari malformation was. It wasn’t until I came to the United States, had a baby and hit a complete rock bottom that I found out that a condition called Chiari even existed.
“But you look so good” is what people usually say when they find out that I struggle with debilitating chronic illnesses. It is true- I wear fashionable clothes, I do my hair, I put on makeup and I have a smile on my face. Underneath it all though, is someone who is trying to live her best life with the cards she was dealt with. I grew up in southern India and none of my family members knew what Chiari malformation was. It wasn’t until I came to the United States, had a baby and hit a complete rock bottom that I found out that a condition called Chiari even existed. with that same narrative, I started questioning if it was all indeed in my mind and psychosomatic. I was starting to accept that living like that was going to be my new normal. I was training with my figure skating coach to be able to make to adult nationals. Skating gave me joy because it was an artistic sport that I could distract myself with. But eventually, the pain took that joy away from me.
with that same narrative, I started questioning if it was all indeed in my mind and psychosomatic. I was starting to accept that living like that was going to be my new normal. I was training with my figure skating coach to be able to make to adult nationals. Skating gave me joy because it was an artistic sport that I could distract myself with. But eventually, the pain took that joy away from me. From the diagnosis of Chiari 1.5 to surgery was about 3 weeks. I liked my surgeon and the care team, so I was comfortable with the surgery. Recovery was long and painful though. I had meningitis twice after the surgery, developed chronic migraines in addition to trigeminal and occipital neuralgia. The diagnosis of central sleep apnea, MCAS and EDS came a year later. My brain stem was traumatized massively. I had to go to vestibular physical rehabilitation therapy to fully walk independently again. A year after my Chiari decompression, I had the Nissen Fundoplication to fix my esophagus. Four years past surgery, I am still recovering and learning how to manage my conditions. My care team now consists of – Anesthesiologist, Physiatrist, Neurologist, Pulmonologist, Gastroenterologist, ENT doctor, Massage Therapists, and Mental Health Counselors in addition to my close family. A huge part of learning how to manage these conditions has been figuring out what my physical limitations are and listening to my body cues. It has taken a long time to learn that it is ok to say no and that it is ok to have a LOT of mental energy but have little to no capacity to do things physically. I gave up figure skating because that kind of physical activity was causing me extreme pain. I get intense urges to skate every now and then which I give into occasionally but as the years have gone by, I am much better at gauging the pain and deciding not to do it. Loud sounds and bright lights trigger a lot of pain now, so I am better about avoiding places that I know are noisy and overwhelming. I have found peace in hiking through the wonderful trails of the pacific northwest. I have cut down on social commitments to prioritize my health over anything else. Some weekends, I do nothing except sleep all day… I have had to learn that that is OK. My husband has been a huge support and my pillar to lean on for the 11 years that we have been married. If I am tempted to do something against my better judgment, he reminds me to know my limitations. I have made peace with the fact that some people might find it impossible to hard to understand what living with Chiari and the comorbid conditions is like and that I cannot control how other people see it. My job has been a stable and joyful part of my life, but it took me a long time to accept that too since my original goal was to go to medical school. I realized my personal limitation about not being able to make it through medical residency. I want to let everyone know that there is hope at the other end of the tunnel… even though it is not in the form of a cure.
From the diagnosis of Chiari 1.5 to surgery was about 3 weeks. I liked my surgeon and the care team, so I was comfortable with the surgery. Recovery was long and painful though. I had meningitis twice after the surgery, developed chronic migraines in addition to trigeminal and occipital neuralgia. The diagnosis of central sleep apnea, MCAS and EDS came a year later. My brain stem was traumatized massively. I had to go to vestibular physical rehabilitation therapy to fully walk independently again. A year after my Chiari decompression, I had the Nissen Fundoplication to fix my esophagus. Four years past surgery, I am still recovering and learning how to manage my conditions. My care team now consists of – Anesthesiologist, Physiatrist, Neurologist, Pulmonologist, Gastroenterologist, ENT doctor, Massage Therapists, and Mental Health Counselors in addition to my close family. A huge part of learning how to manage these conditions has been figuring out what my physical limitations are and listening to my body cues. It has taken a long time to learn that it is ok to say no and that it is ok to have a LOT of mental energy but have little to no capacity to do things physically. I gave up figure skating because that kind of physical activity was causing me extreme pain. I get intense urges to skate every now and then which I give into occasionally but as the years have gone by, I am much better at gauging the pain and deciding not to do it. Loud sounds and bright lights trigger a lot of pain now, so I am better about avoiding places that I know are noisy and overwhelming. I have found peace in hiking through the wonderful trails of the pacific northwest. I have cut down on social commitments to prioritize my health over anything else. Some weekends, I do nothing except sleep all day… I have had to learn that that is OK. My husband has been a huge support and my pillar to lean on for the 11 years that we have been married. If I am tempted to do something against my better judgment, he reminds me to know my limitations. I have made peace with the fact that some people might find it impossible to hard to understand what living with Chiari and the comorbid conditions is like and that I cannot control how other people see it. My job has been a stable and joyful part of my life, but it took me a long time to accept that too since my original goal was to go to medical school. I realized my personal limitation about not being able to make it through medical residency. I want to let everyone know that there is hope at the other end of the tunnel… even though it is not in the form of a cure.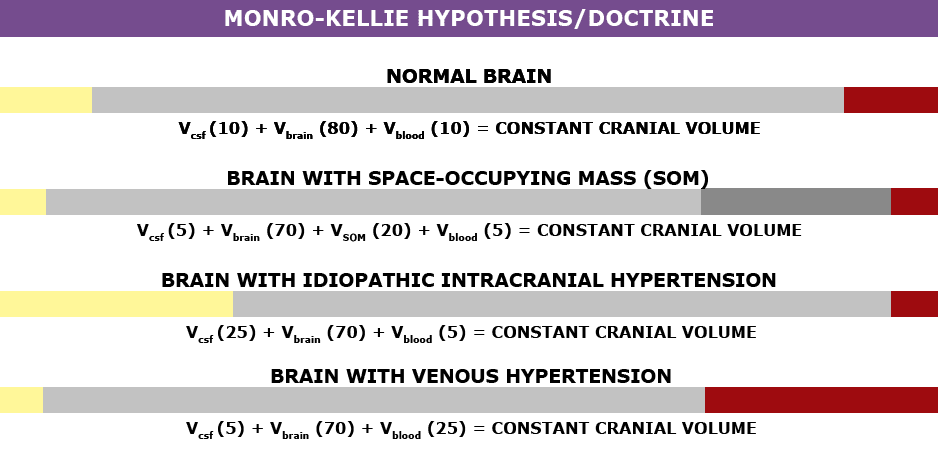



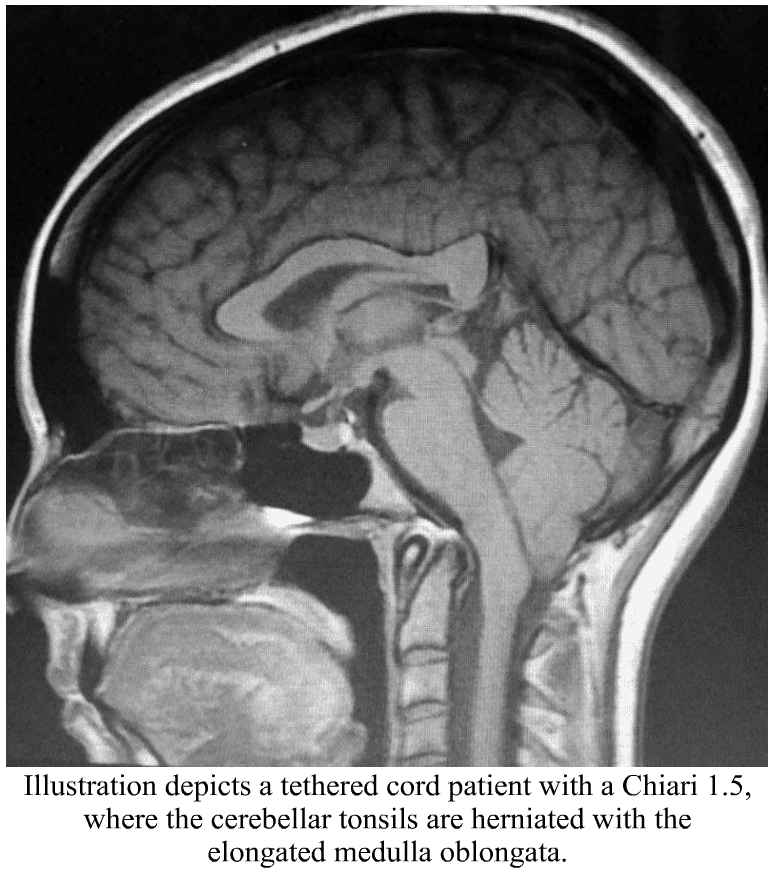 Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.
Chiari Malformation has many conditions that can be associated with it (comorbid conditions) and sometimes those comorbid conditions can be at the root cause (etiological cofactor) or one of the causes along the way (pathological cofactor) to the tonsils being as low as they are (making the Chiari “secondary” to one or more “other” conditions). Tethered Cord Syndrome (TCS) is one of those pathological conditions.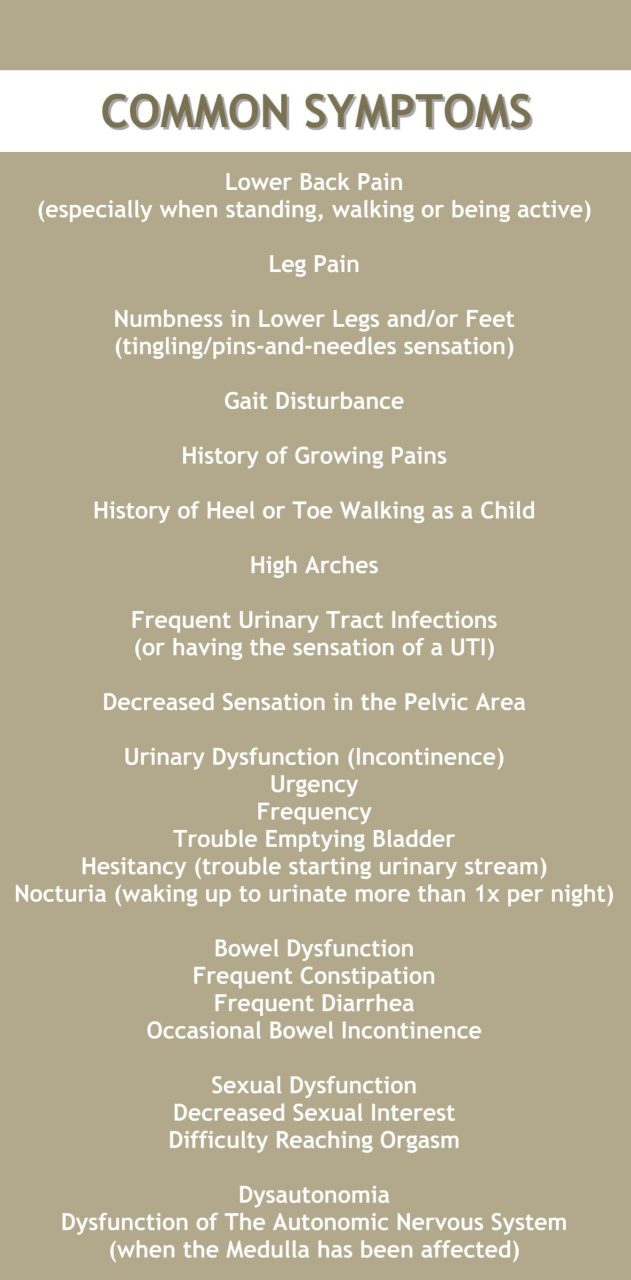
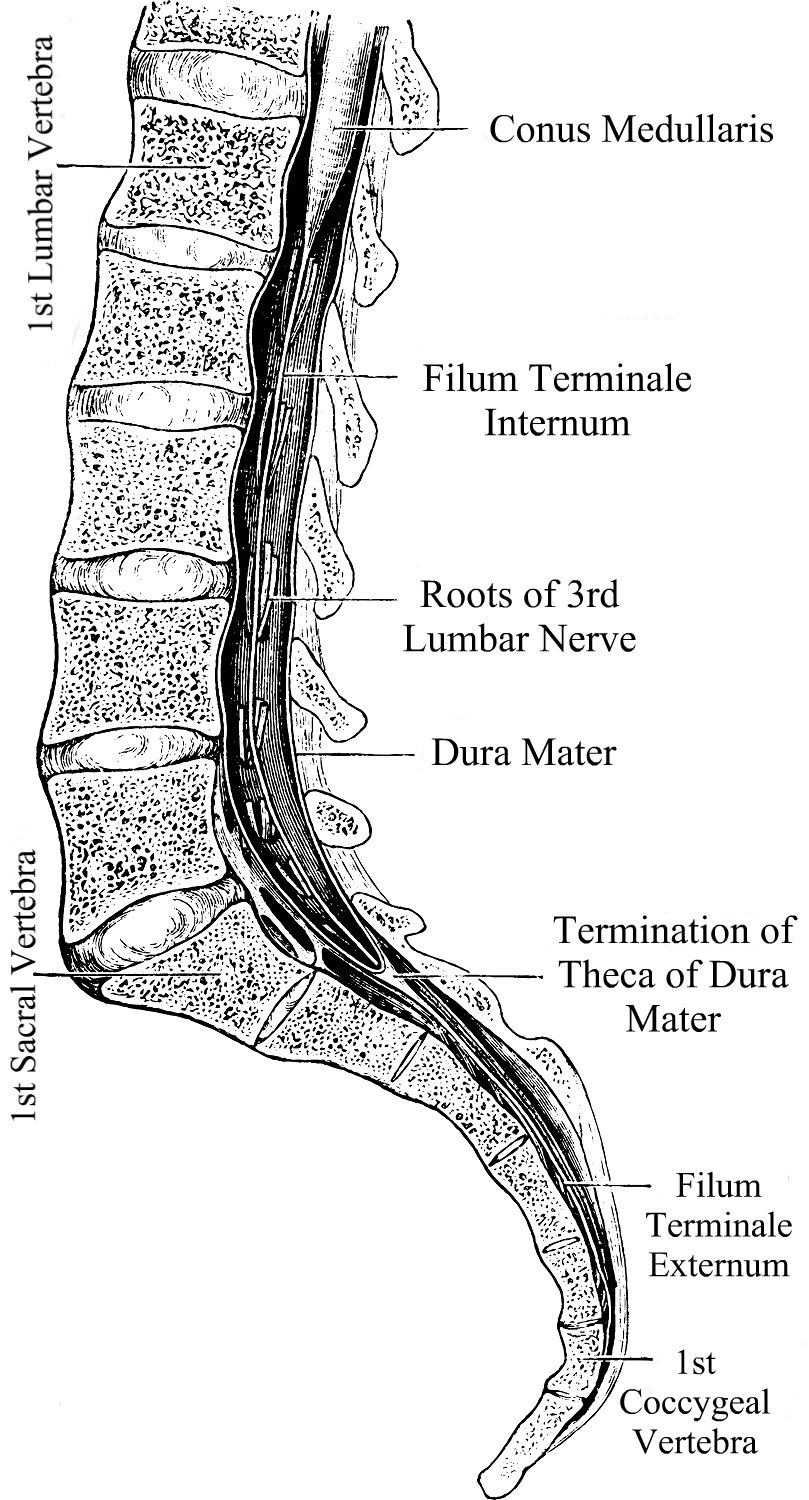 What We Recommend
What We Recommend 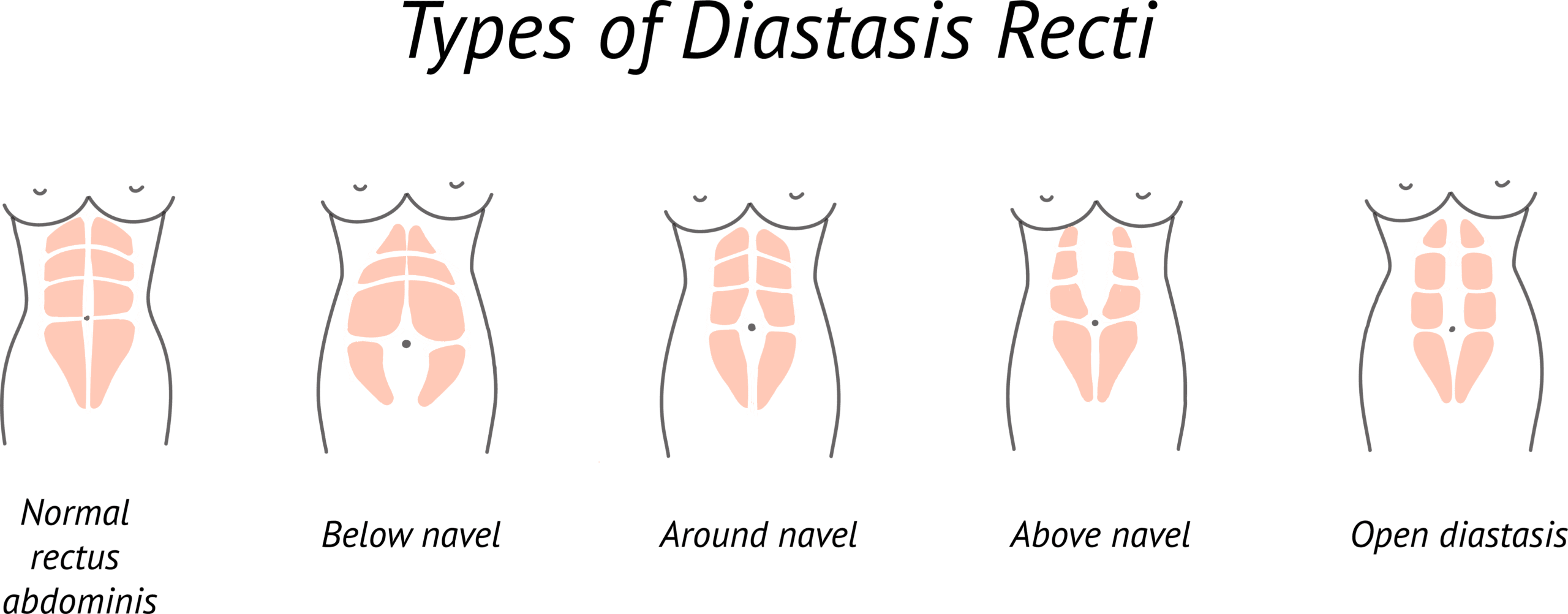


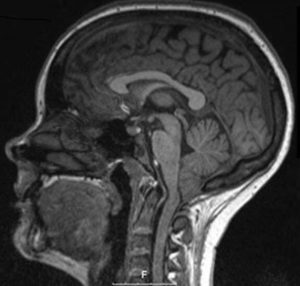 Våren 2017 var jag den lyckligaste människan på jorden. Vi skulle äntligen bli en liten familj. Vi hade längtat och planerat i flera år för en liten människa och till slut kröp pluset fram på stickan. Jag trodde inte jag kunde vara lyckligare än då. Tiden gick och vi levde i vår lyckobubbla. Jag var van vid att få ont i huvudet när jag skrattade, hostade eller nös och trodde att detta var något som hände alla – men helt plötsligt började jag få riktigt ont i huvudet. Läkaren på vårdcentralen sa att det hörde till graviditeten och jag skulle inte oroa mig. Jag försökte ignorera symptomen men de eskalerade snabbt med dålig balans, jag tappade styrka och koordination i armar och ben, såg dubbelt och hade stora svårigheter med minne och koncentration. Till slut gick jag till läkaren igen som nog ändå tyckte att jag skulle till akuten för och magnetröntgas. Jag kunde ju ha fått en hjärnblödning.
Våren 2017 var jag den lyckligaste människan på jorden. Vi skulle äntligen bli en liten familj. Vi hade längtat och planerat i flera år för en liten människa och till slut kröp pluset fram på stickan. Jag trodde inte jag kunde vara lyckligare än då. Tiden gick och vi levde i vår lyckobubbla. Jag var van vid att få ont i huvudet när jag skrattade, hostade eller nös och trodde att detta var något som hände alla – men helt plötsligt började jag få riktigt ont i huvudet. Läkaren på vårdcentralen sa att det hörde till graviditeten och jag skulle inte oroa mig. Jag försökte ignorera symptomen men de eskalerade snabbt med dålig balans, jag tappade styrka och koordination i armar och ben, såg dubbelt och hade stora svårigheter med minne och koncentration. Till slut gick jag till läkaren igen som nog ändå tyckte att jag skulle till akuten för och magnetröntgas. Jag kunde ju ha fått en hjärnblödning. Dagen efter kom överläkaren in till mig. Han berättade att min lillhjärna buktade ut 13mm från skallbasen och att de helst av allt velat skicka mig på operation på en gång eftersom jag hade så svåra besvär, men med tanke på lilla bebisen så fick det lov och vänta tills den var säkert ute. Utanför mitt fönster började världen göra sig redo för sommaren och i kalendern stod det Juni 2017.
Dagen efter kom överläkaren in till mig. Han berättade att min lillhjärna buktade ut 13mm från skallbasen och att de helst av allt velat skicka mig på operation på en gång eftersom jag hade så svåra besvär, men med tanke på lilla bebisen så fick det lov och vänta tills den var säkert ute. Utanför mitt fönster började världen göra sig redo för sommaren och i kalendern stod det Juni 2017. faktiskt inte alls så mycket av den tiden. Det var för mycket att hantera sorgen av både min egen sjukdom och att vårt barn aldrig fick bli. Världen kändes grym och jävlig.
faktiskt inte alls så mycket av den tiden. Det var för mycket att hantera sorgen av både min egen sjukdom och att vårt barn aldrig fick bli. Världen kändes grym och jävlig. I mars 2018 tog läkarna bort 2,5 cm skallben och 2cm på min atlaskota. När jag vaknade så mådde jag bra, förutom att de glömt stänga mitt ena öga innan de la mig nedåt på britsen så det gick sönder (Yes, sånt händer). Det tog ett tag innan det läkte och jag har idag ärr på hornhinnan som aldrig försvinner. Trots ögat så kände jag mig ändå okej, men det hela varade bara i två veckor innan jag fick en kemisk hjärnhinneinflammation och fick ligga inlagd på sjukhus igen. Väl hemma så väntade och väntade jag på att få må bättre, men det hände helt enkelt inte. Huvudvärken var fortfarande jobbig, jag kunde inte ligga på rygg eller bakhuvudet utan att känna som om jag skulle svimma, jag var svag, yr och en hel del neurologiska besvär i form av känselbortfall och smärta. Läkarna försökte alla möjliga mediciner, men allt gav mig biverkningar och ingenting fungerade egentligen. Jag fick välja mellan bisarra svåra biverkningar och att stå på morfin och som du kanske vet så är inte läkare alldeles för förtjusta i opiater mot långvarig smärta. Hur mycket läkarna än försökte justera medicinerna så var det ingenting som jag kunde ta. Jag hade ont.
I mars 2018 tog läkarna bort 2,5 cm skallben och 2cm på min atlaskota. När jag vaknade så mådde jag bra, förutom att de glömt stänga mitt ena öga innan de la mig nedåt på britsen så det gick sönder (Yes, sånt händer). Det tog ett tag innan det läkte och jag har idag ärr på hornhinnan som aldrig försvinner. Trots ögat så kände jag mig ändå okej, men det hela varade bara i två veckor innan jag fick en kemisk hjärnhinneinflammation och fick ligga inlagd på sjukhus igen. Väl hemma så väntade och väntade jag på att få må bättre, men det hände helt enkelt inte. Huvudvärken var fortfarande jobbig, jag kunde inte ligga på rygg eller bakhuvudet utan att känna som om jag skulle svimma, jag var svag, yr och en hel del neurologiska besvär i form av känselbortfall och smärta. Läkarna försökte alla möjliga mediciner, men allt gav mig biverkningar och ingenting fungerade egentligen. Jag fick välja mellan bisarra svåra biverkningar och att stå på morfin och som du kanske vet så är inte läkare alldeles för förtjusta i opiater mot långvarig smärta. Hur mycket läkarna än försökte justera medicinerna så var det ingenting som jag kunde ta. Jag hade ont. Min främsta fiende var nu tiden och den sniglade sig fram. Snart var det februari 2019. 11 månader efter att jag fått min första operation. Jag kunde inte längre klara av en vardag, jag sov mestadels under dagarna och jag hade så väldigt ont. Min sambo tog hand om hemmet och mig. När jag låg på rygg så svimmade jag och livet var outhärdligt. Jag skrev återigen ett meddelande till min kirurg och denna gång tog jag helt enkelt farväl. Jag kände hur livet rann ur mig och det fanns snart inte mer tid kvar. Han ringde upp nästan på en gång och berättade att de nu tänkte göra en till operation. De hade fortfarande inga indikationer och ville göra några tester innan jag fick operationstid. Jag fick göra neurologiska tester, en magnetröntgen och en lumbalpunktion för att kolla trycket i skallen. Magnetröntgen fick jag göra under narkos eftersom att jag inte kunde ligga på bakhuvudet och tryckmätningen visade att mitt tryck låg lite högt. Neurologen tyckte att jag var tjock med ett par kilo extra för min längd så de la inte någon vikt vid resultaten men efter testerna så fick jag tid för operation igen. April 2019.
Min främsta fiende var nu tiden och den sniglade sig fram. Snart var det februari 2019. 11 månader efter att jag fått min första operation. Jag kunde inte längre klara av en vardag, jag sov mestadels under dagarna och jag hade så väldigt ont. Min sambo tog hand om hemmet och mig. När jag låg på rygg så svimmade jag och livet var outhärdligt. Jag skrev återigen ett meddelande till min kirurg och denna gång tog jag helt enkelt farväl. Jag kände hur livet rann ur mig och det fanns snart inte mer tid kvar. Han ringde upp nästan på en gång och berättade att de nu tänkte göra en till operation. De hade fortfarande inga indikationer och ville göra några tester innan jag fick operationstid. Jag fick göra neurologiska tester, en magnetröntgen och en lumbalpunktion för att kolla trycket i skallen. Magnetröntgen fick jag göra under narkos eftersom att jag inte kunde ligga på bakhuvudet och tryckmätningen visade att mitt tryck låg lite högt. Neurologen tyckte att jag var tjock med ett par kilo extra för min längd så de la inte någon vikt vid resultaten men efter testerna så fick jag tid för operation igen. April 2019. I dagsläget när jag skriver detta så vet man inte någonting egentligen gällande mig. Varför allt är som det är och varför jag blir så sjuk. Jag är ett stort frågetecken hos sjukvården, så jag gör vad vi måste göra i denna situation. Jag läser på, pluggar och kämpar. Vågar fråga och är jobbig. Jag tar hjälp av personer som går i samma skor som jag och utan communityn på Facebook så vet jag inte vad jag hade gjort. Jag svarar på frågor jag inte borde behöva svara på när jag kommer till vårdcentral eller sjukhus ”Vad sa du att du hade sa du?” , men jag hade inte orkat kämpa om jag inte haft känslan av att jag inte är själv. Jag tror inte att någonting kan hända mig nu som jag inte redan gått igenom, men skillnaden nu är att jag har mer kunskap och erfarenhet men jag är också utmattad, trött och stundtals nedslagen av att behöva slåss. Att gå igenom så pass stora och allvarliga operationer utan att bli frisk är inte helt lätt att hantera alla dagar. Man ska ju liksom inte bli lika dålig, om inte sämre – efteråt. Man ska ju bli botad.
I dagsläget när jag skriver detta så vet man inte någonting egentligen gällande mig. Varför allt är som det är och varför jag blir så sjuk. Jag är ett stort frågetecken hos sjukvården, så jag gör vad vi måste göra i denna situation. Jag läser på, pluggar och kämpar. Vågar fråga och är jobbig. Jag tar hjälp av personer som går i samma skor som jag och utan communityn på Facebook så vet jag inte vad jag hade gjort. Jag svarar på frågor jag inte borde behöva svara på när jag kommer till vårdcentral eller sjukhus ”Vad sa du att du hade sa du?” , men jag hade inte orkat kämpa om jag inte haft känslan av att jag inte är själv. Jag tror inte att någonting kan hända mig nu som jag inte redan gått igenom, men skillnaden nu är att jag har mer kunskap och erfarenhet men jag är också utmattad, trött och stundtals nedslagen av att behöva slåss. Att gå igenom så pass stora och allvarliga operationer utan att bli frisk är inte helt lätt att hantera alla dagar. Man ska ju liksom inte bli lika dålig, om inte sämre – efteråt. Man ska ju bli botad. When I first started getting hit with symptoms, I was a divorced, single mother of three amazing kids; responsible not only to provide for them but to see them through life, unscathed by life’s situations, and showing them that there was nothing that if they worked hard at something, nothing could hold them back. I had just started to expand in my career as a self-taught auto technician. I was a woman making a place for herself in an industry traditionally dominated by males. July 3, 2015, was the day that my life forever changed. I was brought to the hospital with stroke-like symptoms. I was having visual problems. I couldn’t walk or talk. I had no idea who I was or where I was. The whole right side of my body basically stopped working and the right side of my face was droopy. I was brought to the ER and before the doctor would even try to figure out what was wrong with me, he ordered a series of drug tests. I passed every test, so he finally admitted to me. Once on the neurology floor, more testing was done. They performed an MRI, MRA, EKG and told us that all results were normal. I later discovered that was not the case.
When I first started getting hit with symptoms, I was a divorced, single mother of three amazing kids; responsible not only to provide for them but to see them through life, unscathed by life’s situations, and showing them that there was nothing that if they worked hard at something, nothing could hold them back. I had just started to expand in my career as a self-taught auto technician. I was a woman making a place for herself in an industry traditionally dominated by males. July 3, 2015, was the day that my life forever changed. I was brought to the hospital with stroke-like symptoms. I was having visual problems. I couldn’t walk or talk. I had no idea who I was or where I was. The whole right side of my body basically stopped working and the right side of my face was droopy. I was brought to the ER and before the doctor would even try to figure out what was wrong with me, he ordered a series of drug tests. I passed every test, so he finally admitted to me. Once on the neurology floor, more testing was done. They performed an MRI, MRA, EKG and told us that all results were normal. I later discovered that was not the case. A few days later, I followed up with my PCP. She went over my MRI results with me and pointed out that they found a Chiari Malformation with a 19mm herniation of my cerebellar tonsils. She told me of changes in my white matter that the radiologist said needed to be “further evaluated” and referred me to my first neurologist, who I met within August. He ordered a visual evoked potential and an EEG. Both come back normal, so he diagnosed me with migraines, even after hearing my symptoms, which frustrates me even more as I know that it is not migraines causing these issues.
A few days later, I followed up with my PCP. She went over my MRI results with me and pointed out that they found a Chiari Malformation with a 19mm herniation of my cerebellar tonsils. She told me of changes in my white matter that the radiologist said needed to be “further evaluated” and referred me to my first neurologist, who I met within August. He ordered a visual evoked potential and an EEG. Both come back normal, so he diagnosed me with migraines, even after hearing my symptoms, which frustrates me even more as I know that it is not migraines causing these issues. During this care for MS, I kept having what they thought were MS relapses, roughly every three to four months. Each time they ordered new MRI images and treated me with high doses of IV steroids for five days in a row. Never once did this imaging ever show an actual MS-relapse or MS activity. I continually had issues with every medication that they put me on to help “try to delay the progression of the MS” (the MS that I never had). In November 2017 I started Ocrevus, which was just FDA approved that year. Around this time, I started having strange symptoms and thought them just to be side effects of the medication, not realizing that something else might be causing it all. I met with my neurologist before my second full dose and I told her everything that I was experiencing. We opted to take me off the Ocrevus and they repeated the MRI yet again. Again, the MRIs show absolutely nothing new for activity and she admits that she doesn’t know what to do for me. I am three years in at that point and never once have they seen any MS activity.
During this care for MS, I kept having what they thought were MS relapses, roughly every three to four months. Each time they ordered new MRI images and treated me with high doses of IV steroids for five days in a row. Never once did this imaging ever show an actual MS-relapse or MS activity. I continually had issues with every medication that they put me on to help “try to delay the progression of the MS” (the MS that I never had). In November 2017 I started Ocrevus, which was just FDA approved that year. Around this time, I started having strange symptoms and thought them just to be side effects of the medication, not realizing that something else might be causing it all. I met with my neurologist before my second full dose and I told her everything that I was experiencing. We opted to take me off the Ocrevus and they repeated the MRI yet again. Again, the MRIs show absolutely nothing new for activity and she admits that she doesn’t know what to do for me. I am three years in at that point and never once have they seen any MS activity. The last four years have been one hell of a ride when it comes to my health. My health problems have made it far more difficult to continue working on cars. As my symptoms wage war on my body, I am now forced to work on light duty and have been for the last two and a half years. I know that my days of working in a shop are coming to end as I just can’t handle the physical requirements of the job anymore. My quality of life in the last year alone has declined sharply. I used to be the energetic mom who could coach a sports team after working all day in the shop and still have the energy to keep up with the housework, now that is not the case. I manage to push on and get them to their activities, but I’m exhausted to the core. When this all began back in 2015 my kids were 8, 7, and 5. They are now 12, 11 and 9. At times I feel like I am a horrible mother because I miss the mom that I used to be. I miss the days when my kids weren’t worried about my health and when we could make plans with other families and keep them. I have lost so much of who I am thanks to the ignorance of some members of the medical community. I am losing faith in the medical profession in general. Male doctors have been the worst as I go through this journey, as women seem to have to first prove that it’s not psychosomatic before we’re worthy of being helped, even with imaging shows something to the contrary. When I present them with proven facts about Chiari Malformation, it still gets dismissed and it is extremely frustrating. The longer I go without receiving proper treatment, the more likely it becomes that some of this damage will become permanent and to me, that is not acceptable. I am fighting for my life and I will not back down until I receive the proper care, I can’t!
The last four years have been one hell of a ride when it comes to my health. My health problems have made it far more difficult to continue working on cars. As my symptoms wage war on my body, I am now forced to work on light duty and have been for the last two and a half years. I know that my days of working in a shop are coming to end as I just can’t handle the physical requirements of the job anymore. My quality of life in the last year alone has declined sharply. I used to be the energetic mom who could coach a sports team after working all day in the shop and still have the energy to keep up with the housework, now that is not the case. I manage to push on and get them to their activities, but I’m exhausted to the core. When this all began back in 2015 my kids were 8, 7, and 5. They are now 12, 11 and 9. At times I feel like I am a horrible mother because I miss the mom that I used to be. I miss the days when my kids weren’t worried about my health and when we could make plans with other families and keep them. I have lost so much of who I am thanks to the ignorance of some members of the medical community. I am losing faith in the medical profession in general. Male doctors have been the worst as I go through this journey, as women seem to have to first prove that it’s not psychosomatic before we’re worthy of being helped, even with imaging shows something to the contrary. When I present them with proven facts about Chiari Malformation, it still gets dismissed and it is extremely frustrating. The longer I go without receiving proper treatment, the more likely it becomes that some of this damage will become permanent and to me, that is not acceptable. I am fighting for my life and I will not back down until I receive the proper care, I can’t!